[level-membership-for-dermatology-category]
30 Tattoo Removal with Lasers
The growing trend of tattooing has led to increased numbers of patients seeking tattoo removal. Studies note that 40% of Americans between the age of 26 and 40 currently have tattoos and 17% of these people are seeking removal.1,2 With more than 20,000 tattoo studios in the United States placing tattoos, the demand for removal is likely to continue to increase in the coming years.3
Multiple techniques can be used for tattoo removal. Early removal methods used mechanical destruction such as dermabrasion, chemical peels, and continuous-wave lasers. These methods left patients with unsatisfactory results and were associated with suboptimal removal and scarring (Figure 30-1). The current standard of using Q-switched lasers has revolutionized tattoo removal and offers patients a safe and effective means for removing tattoo ink.

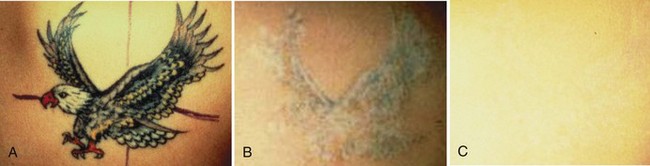
FIGURE 30-1 Dermabrasion results for tattoo removal showing scarring, hypopigmentation, and residual ink.
(Copyright Rebecca Small, MD.)
Tattoo Anatomy
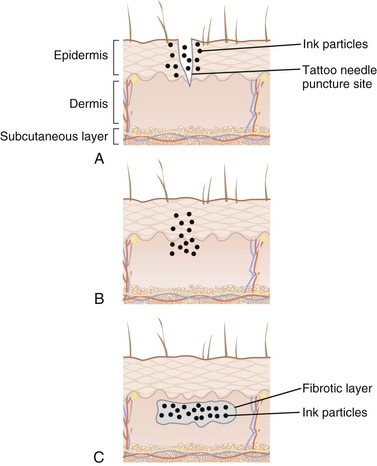
During the tattooing process, tattoo ink is injected intradermally. The epidermis and upper papillary dermis are homogenized and ink particles (ranging in size from 2 to 400 nm) are deposited intracellularly and extracellularly. After 2 to 3 months, the skin layers are reestablished and ink is concentrated in the dermis within fibroblasts, beneath a layer of fibrotic scar tissue (Figure 30-2).
Laser Principles
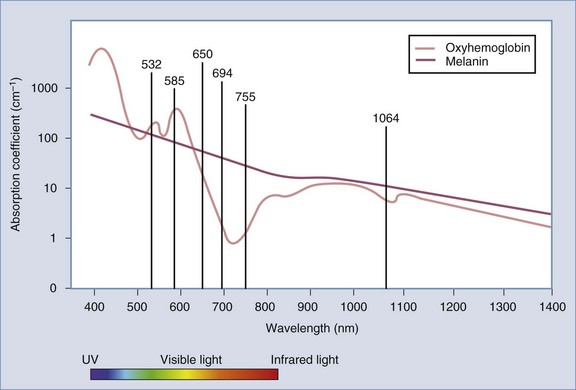
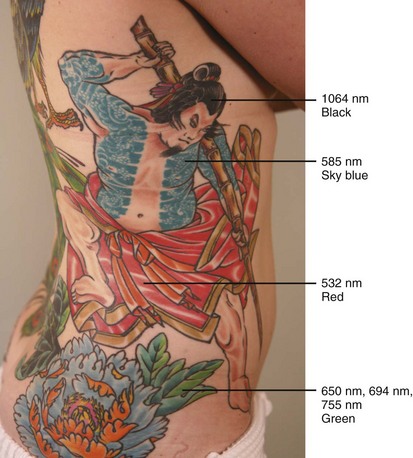
Tattoo ink serves as a cutaneous chromophore for lasers. Certain wavelengths of light are selectively absorbed by different ink colors.4 In this way, colored inks can be targeted and removed by laser light with minimal damage to surrounding tissues. The chromophore absorption spectrum of the tissue chromophores, melanin and oxyhemoglobin, as well as wavelengths used for tattoo removal, are shown in Figure 30-3. Wavelength selection for different tattoo colors is shown in Figure 30-4 and is as follows:
Laser parameters including wavelength, pulse duration, and fluence can be tailored to maximize tattoo ink destruction and minimize thermal damage to surrounding tissue. Short pulsed, Q-switched lasers further employ photoacoustic vibration to fragment tattoo ink into smaller particles. These smaller ink particles are eliminated through epidermal extrusion, lymphatic drainage, and macrophage phagocytosis. In addition, laser-treated ink particles have altered optical properties that render the ink remaining in the skin less visible to the eye.5
Laser Parameters and Tattoo Treatments
Patient and Tattoo Selection
Almost any tattoo is indicated for laser tattoo removal. Multiple treatments are needed to achieve satisfactory results. Due to great variation in tattoo ink depth, density, composition, and techniques used for placement, the number of treatments needed for removal can be difficult to estimate accurately. In general, professionally placed tattoos have a high ink density and require 9 to 14 treatments, whereas amateur tattoos typically require 4 to 8 treatments. Several other factors can affect the number of treatments necessary for removal: faded, older tattoos on paler skin types in more proximal locations tend to resolve with fewer treatments than intense, multicolored tattoos on darker skin types in distal locations.6 Patients should be questioned about other tattoo removal methods used previously. Methods that create scar tissue, such as burning or abrasion, can make tattoo removal with lasers less successful.
Alternative Therapies
The following alternatives to Q-switched laser tattoo removal methods are not recommended:
Products Currently Available
The Q-switched Nd:YAG (neodymium-doped yttrium aluminum garnet) produces a 1064 nm wavelength of light that is ideal for treating black ink. A primary disadvantage is its limited efficacy in removing yellow and green inks. With some devices, through a process called frequency doubling, an Nd:YAG laser can also produce light with a wavelength of 532 nm to treat red, orange, and yellow inks.20 The Nd:YAG laser has an advantage of treating darker skinned patients with less risk of hypopigmentation, hyperpigmentation, and textural changes.7 This can be attributed to the increased dermal penetration of this longer wavelength and the lower melanin absorption. The wavelength of the light emitted by the Q-switched alexandrite laser is 755 nm. This wavelength has excellent absorption by black, good absorption by green and blue, but poor absorption by red ink. The ruby laser was one of the first Q-switched lasers, and it emits a 694 nm wavelength. It works well for darker colors (black, blue-black, and some green), but poorly on yellow and red ink. Although more effective for green ink than the Nd:YAG, the ruby laser commonly causes hypopigmentation and hyperpigmentation and, although usually transient, may be permanent.5
Contraindications8
Also see Chapter 26, Hair Reduction with Lasers, for additional laser contraindications.
Procedure Preparation

Laser Tattoo Removal: Steps and Principles
General Treatment Technique
Anesthesia
Tattoo treatments are painful but can be performed relatively quickly. Some patients may forgo anesthesia altogether, but many patients require some form of local anesthesia. A topical anesthetic cream such as benzocaine:lidocaine:tetracaine (see the Resources list at the end of the chapter) may be used under occlusion with plastic wrap for 30 minutes in the office prior to the laser treatment. If complete anesthesia is desired, injections of 1% or 2% lidocaine with epinephrine subdermally may be used. Local injection is discouraged by the authors because clinical experience has shown increased bleeding and edema at the time of treatment, rendering treatments less effective.
Performing the Procedure

Results
Immediately after a Q-switched laser treatment, the tattoo will have a white discoloration. Figure 30-6 shows a blue-black tattoo during treatment with immediate whitening. This white color change is thought to be the result of rapid, heat-formed steam, causing dermal and epidermal vacuolization. Patients may perceive this as reduction of ink, but this positive change is only temporary and typically lasts for 20 minutes or less. Ink color will gradually fade during the month following each treatment. Results from laser treatments for removal of tattoo ink are cumulative and results from some treatments will be more noticeable than others.
Figure 30-7 shows a blue-black professional tattoo (A) before and (B) after five treatments with a Q-switched laser using 1064 nm wavelength (HOYA ConBio Medlite) demonstrating typical tattoo clearance. Figure 30-8 shows a multicolor professional tattoo (A) before, (B) midway through treatment with lightening of the black ink and hypopigmentation, and (C) after completion of treatment with a Q-switched laser using 1064, 532, and 585 nm wavelengths for black/blue, red/yellow, and sky blue inks, respectively (HOYA ConBio Medlite).

Occasionally colored inks may darken with treatment due to darker constituent inks. Figure 30-9A shows a red ink tattoo prior to treatment. This tattoo was initially treated with a Q-switched laser using a 1064 nm wavelength (Medlite, Hoya ConBio) and the tattoo ink darkened and became black in color (Figure 30-9B). Subsequent treatments were performed using a 1064 nm wavelength for black and a 532 nm wavelength for red ink areas.

Complications
A fine line exists between expected side effects and true complications from laser tattoo removal treatments. For example, discomfort, swelling, blistering, and itching are commonly associated with the treatment8 but extreme pain, limb edema, bulla, and intractable pruritus are rare and indicate treatment complications.
About half of the patients treated with Q-switched lasers for tattoo removal will show some transient changes in the normal skin pigmentation (hyperpigmentation or hypopigmentation).5,9 These changes usually resolve in 6 to 12 months but rarely may be permanent.7,10 The risk of hyperpigmentation and hypopigmentation is greatest with skin types IV, V, and VI, regardless of the wavelength used. Areas that blister and bleed are more likely to have pigmentary and textural changes.11 Twice daily treatment with hydroquinone and broad-spectrum sunscreens on fully healed skin usually resolve hyperpigmentation within a few months, although in some patients resolution can be prolonged. Shorter wavelengths, such as 532 nm, are more commonly associated with blistering and hypopigmentation than longer wavelengths.
Transient textural changes are common and typically resolve within a few months; however, permanent textural changes and scarring can occur.10 If a patient is prone to pigmentary or textural changes, longer treatment intervals are recommended. Additionally, patients with a history of hypertrophic scarring need to be warned of their increased risk of scarring.
Local allergic responses to tattoo pigments have been reported at the time of tattoo placement, and allergic reactions to tattoo pigment can also occur after Q-switched laser treatment.13–18 For example, photoallergic reactions have been reported to yellow cadmium sulfide, a pigment commonly added to tattoos to brighten red or yellow inks. This reaction is also reported with red ink, which may contain cinnabar (mercuric sulfide), green (chromium), and blue (cobalt).21,22 Erythema, pruritus, and even inflamed nodules, verrucose papules, or granulomas may occur. The reaction is confined to the site of the red/yellow ink. Treatment consists of strict sunlight avoidance, use of sunscreen, intralesional steroid injections, or in some cases, surgical removal.22 Q-switched lasers mobilize the ink through the lymphatic system and systemic allergic responses are extremely rare complications. Oral antihistamines and anti-inflammatory steroids may also be used to treat allergic reactions to tattoo ink.23
Treating Specific Lesions
Caution should be used with cosmetic ink appearing pink, flesh colored, or peach because these may contain iron oxide or titanium oxide pigments.25 These pigments, when treated with a Q-switched laser, may turn brown or black in a phenomenon known as paradoxical darkening.9 Although this brown or black color usually responds well to continued treatment, it can be disconcerting to patients as the effect of early treatment will often leave the tattoo looking darker than it did prior to treatment. If tattoo darkening does occur, after 8 weeks, the newly darkened tattoo can be treated as if it were black pigment with 1064 nm.
Traumatic tattoos resulting from asphalt or “road rash” can be effectively treated with laser tattoo removal methods.24 Obtaining a proper history is imperative when treating any traumatic tattoo because case reports of laser ignition from flammable debris have been reported.12,26
Financial Considerations
Although tattooing of skin may be considered medically necessary when performed as part of a therapeutic intervention (e.g., radiation therapy, or with breast reconstruction), tattoo removal is considered cosmetic and is not reimbursed by insurance providers. Most providers base their fee for tattoo removal on the size of the tattoo and the presence or absence of multiple colors. For example, fees for black tattoos less than or equal to 9 in.2 may be $200; 10 to 25 in.2, $350; and 26 to 49 in.2, $500; with an additional $100 added for tattoos containing red, sky blue, or green.
1. Farmer S, Laumann A, Baranwal M. Epidemiology of tattooing and body piercing: National Data Set. J Am Acad Dermatol. 2005;52:104.
2. Harris RB. Harris Poll. 2003:58.
3. Mariwalla K, Dover JS. The use of lasers for decorative tattoo removal. Skin Ther Lett. 2006;11:8-11.
4. Kirby W, Desai A, Kartono F. Tattoo removal techniques: effective tattoo removal treatments—Part I. Skin and Aging. 2005;9:50-54.
5. Kilmer SL, Lee MS, Grevelink JM, et al. The Q-switched Nd:YAG laser effectively treats tattoos. A controlled, dose-response study. Arch Dermatol. 1993;129(8):971-978.
6. Kirby W, Desai A, Desai T, et al. The Kirby-Desai scale: A proposed scale to assess tattoo removal treatments. J Clin Aesthetic Dermatol. 2009;2(3):32-37.
7. Grevelink JM, Duke D, van Leeuwen RL, et al. Laser treatment of tattoos in darkly pigmented patients: efficacy and side effects. J Am Acad Dermatol. 1996;34(4):653-656.
8. Crawford K. Laser devices: tattoo removal. In Pfenninger JL, Fowler GC, editors: Pfenninger and Fowler’s Procedures for Primary Care, 3rd ed, Philadelphia: Mosby/Elsevier, 2011.
9. Anderson RR, Geronemus RG, Kilmer SL, et al. Cosmetic tattoo ink darkening. A complication of Q-switched and pulsed-laser treatment. Arch Dermatol. 1993;129:1010-1014.
10. Ho WS, Ying SP, Chan PC, Chan HH. Use of onion extract, heparin, allantoin gel in prevention of scarring in Chinese patients having laser removal of tattoos: a prospective randomized controlled trial. Dermatol Surg. 2006;32(7):891-896.
11. Wenzel SM. Current concepts in laser tattoo removal. Skin Therapy Lett. 2010;15(3):3-5.
12. Fusade T, Toubel G, Grognard C, et al. Treatment of gunpowder traumatic tattoo by Q-switched Nd:YAG laser: an unusual adverse effect. Dermatol Surg. 2000;26(11):1057-1059.
13. England R. Immediate cutaneous hypersensitivity after treatment of tattoo with Nd:YAG laser: a case report and review of the literature. Ann Allergy Asthma Immunol. 2002;89:215-217.
14. McFadden N, Lyberg T, Hensten-Pettersen A. Aluminum-induced granulomas in a tattoo 31. J Am Acad Dermatol. 1989;20(5 Pt 2):903-908.
15. Bagnato G, De Pasquale R, Glacobbe O, et al. Urticaria in a tattooed patient. Allergol et Immunopathol. 1992;71:70-73.
16. Winkelmann RK, Harris RB. Lichenoid delayed hypersensitivity reactions in tattoos. J Cutan Pathol. 1979;6(1):59-65.
17. Bendsoe N, Hansson C, Sterner O. Inflammatory reactions from organic pigments in red tattoos. Acta Dermatol Venereol. 1991;71(1):70-73.
18. Blumental G, Okun MR, Ponitch JA. Pseudolymphomatous reaction to tattoos. Report of three cases. J Am Acad Dermatol. 1982;6(4 Pt 1):485-488.
19. Tazelaar DJ. Hypersensitivity to chromium in a light-blue tattoo. Dermatologica. 1970;141(4):282-287.
20. Kilmer SL, Anderson RR. Clinical use of the Q-switched ruby and the Q-switched Nd:YAG (1064 nm and 532 nm) lasers for treatment of tattoos. J Dermatol Surg Oncol. 1993;19(4):330-338.
21. Bjornberg A. Allergic reactions to chrome in green tattoo markings. Acta Dermatol Venereol. 1959;39(1):23-29.
22. Bjornberg A. Allergic reaction to cobalt in light-blue tattoo markings. Acta Dermatol Venereol. 1961;41:259.
23. Ashinoff R, Levine VJ, Soter NA. Allergic reactions to tattoo pigment after laser treatment. Dermatol Surg. 1995;21:291-294.
24. Agneta M. Effective treatment of traumatic tattoos with a q-switched Nd:YAG laser. Lasers Surg Med. 1998;22:103-108.
25. Lee CN, Bae EY, Park JG, et al. Permanent makeup removal using Q-swiltched Nd:YAG laser. Clin Exp Dermatol. 2009;34(8):e594-e596.
26. Taylor CR. Laser ignition of traumatically embedded firework debris. Lasers Surg Med. 1998;22(3):157-158.
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
30 Tattoo Removal with Lasers
The growing trend of tattooing has led to increased numbers of patients seeking tattoo removal. Studies note that 40% of Americans between the age of 26 and 40 currently have tattoos and 17% of these people are seeking removal.1,2 With more than 20,000 tattoo studios in the United States placing tattoos, the demand for removal is likely to continue to increase in the coming years.3
Multiple techniques can be used for tattoo removal. Early removal methods used mechanical destruction such as dermabrasion, chemical peels, and continuous-wave lasers. These methods left patients with unsatisfactory results and were associated with suboptimal removal and scarring (Figure 30-1). The current standard of using Q-switched lasers has revolutionized tattoo removal and offers patients a safe and effective means for removing tattoo ink.
FIGURE 30-1 Dermabrasion results for tattoo removal showing scarring, hypopigmentation, and residual ink.
(Copyright Rebecca Small, MD.)
Tattoo Anatomy
During the tattooing process, tattoo ink is injected intradermally. The epidermis and upper papillary dermis are homogenized and ink particles (ranging in size from 2 to 400 nm) are deposited intracellularly and extracellularly. After 2 to 3 months, the skin layers are reestablished and ink is concentrated in the dermis within fibroblasts, beneath a layer of fibrotic scar tissue (Figure 30-2).
Laser Principles
Tattoo ink serves as a cutaneous chromophore for lasers. Certain wavelengths of light are selectively absorbed by different ink colors.4 In this way, colored inks can be targeted and removed by laser light with minimal damage to surrounding tissues. The chromophore absorption spectrum of the tissue chromophores, melanin and oxyhemoglobin, as well as wavelengths used for tattoo removal, are shown in Figure 30-3. Wavelength selection for different tattoo colors is shown in Figure 30-4 and is as follows:
Laser parameters including wavelength, pulse duration, and fluence can be tailored to maximize tattoo ink destruction and minimize thermal damage to surrounding tissue. Short pulsed, Q-switched lasers further employ photoacoustic vibration to fragment tattoo ink into smaller particles. These smaller ink particles are eliminated through epidermal extrusion, lymphatic drainage, and macrophage phagocytosis. In addition, laser-treated ink particles have altered optical properties that render the ink remaining in the skin less visible to the eye.5
Laser Parameters and Tattoo Treatments
Patient and Tattoo Selection
Almost any tattoo is indicated for laser tattoo removal. Multiple treatments are needed to achieve satisfactory results. Due to great variation in tattoo ink depth, density, composition, and techniques used for placement, the number of treatments needed for removal can be difficult to estimate accurately. In general, professionally placed tattoos have a high ink density and require 9 to 14 treatments, whereas amateur tattoos typically require 4 to 8 treatments. Several other factors can affect the number of treatments necessary for removal: faded, older tattoos on paler skin types in more proximal locations tend to resolve with fewer treatments than intense, multicolored tattoos on darker skin types in distal locations.6 Patients should be questioned about other tattoo removal methods used previously. Methods that create scar tissue, such as burning or abrasion, can make tattoo removal with lasers less successful.
Alternative Therapies
The following alternatives to Q-switched laser tattoo removal methods are not recommended:
Products Currently Available
The Q-switched Nd:YAG (neodymium-doped yttrium aluminum garnet) produces a 1064 nm wavelength of light that is ideal for treating black ink. A primary disadvantage is its limited efficacy in removing yellow and green inks. With some devices, through a process called frequency doubling, an Nd:YAG laser can also produce light with a wavelength of 532 nm to treat red, orange, and yellow inks.20 The Nd:YAG laser has an advantage of treating darker skinned patients with less risk of hypopigmentation, hyperpigmentation, and textural changes.7 This can be attributed to the increased dermal penetration of this longer wavelength and the lower melanin absorption. The wavelength of the light emitted by the Q-switched alexandrite laser is 755 nm. This wavelength has excellent absorption by black, good absorption by green and blue, but poor absorption by red ink. The ruby laser was one of the first Q-switched lasers, and it emits a 694 nm wavelength. It works well for darker colors (black, blue-black, and some green), but poorly on yellow and red ink. Although more effective for green ink than the Nd:YAG, the ruby laser commonly causes hypopigmentation and hyperpigmentation and, although usually transient, may be permanent.5
Contraindications8
Also see Chapter 26, Hair Reduction with Lasers, for additional laser contraindications.
