53
Syphilis
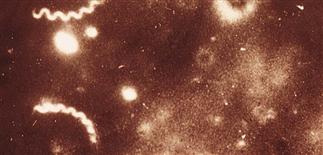
Treponema pallidum is the organism responsible for syphilis. Here, it is seen through a dark-field microscope as a tightly coiled simple bacteria. It is a member of the Spirochete family of bacteria.

Primary syphilis. Lesion begins as papule that undergoes ischemic necrosis and erodes to form a 0.3- to 2.0-cm, painless to tender, hard, indurated ulcer. Base clean with scant yellow serous discharge.

Secondary syphilis, with the characteristic findings of pink oval scaly patches on the palm with slight hyperpigmentation. These findings may also be seed the plantar feet.

Lesions of secondary syphilis have marked tendency to polymorphism, with various types of lesions presenting simultaneously. They have a coppery tint and assume various shapes.
DESCRIPTION
Syphilis (lues) is an infectious disease caused by the spirochete Treponema pallidum. Spread sexually. Can affect virtually every organ. Untreated, syphilis passes through stages: primary, secondary, latent, tertiary.
HISTORY
• Primary. Chancre acquired by direct contact. It appears 21 days after exposure and is usually solitary. Primary chancres resolve but the spirochete remains. • Secondary. Begins 6 weeks after the chancre and results from hematogenous and lymphatic spread of the spirochete. An influenza-like syndrome with mucocutaneous lesions, hepatosplenomegaly, and generalized adenopathy occurs and lasts 2–10 weeks. Skin changes of this stage are easily confused with other skin diseases, especially pityriasis rosea. • Latent. Results of serologic tests are positive without evidence of active disease. Tertiary. Characterized by small number of spirochetes eliciting a large or brisk cellular immune response. This manifests as cardiovascular and central nervous system granulomas or gummas. • Congenital. Yet another variant.
PHYSICAL FINDINGS
• Primary. Chancre is painless and begins as a 3-mm to 2-cm papule, undergoes ischemic necrosis, and erodes. Occasionally it is tender, firm, and indurated. Borders are raised, smooth, sharply defined. Syphilitic chancres on the cervix may be asymptomatic and undetected, may allow transmission. Painless, non-suppurative regional lymphadenopathy develops in 1–2 weeks. • Secondary. Characterized by systemic, cutaneous, and mucosal signs and symptoms. Fever, malaise, pharyngitis, adenopathy, weight loss, and meningeal signs (headache) common. Most common sign is a non-pruritic, generalized, pink, scaly, papular eruption in 80% of patients. Symmetric, hyperpigmented, oval papules with a collarette of scale appear on palms or soles in most patients. Irregular alopecia of beard, scalp, and eyelashes occurs—sometimes referred to as ‘moth-eaten alopecia’. Moist, anal, condyloma lata lesions are highly infectious wart-like papules characteristic of syphilis. All secondary lesions are infectious with direct contact or palpation. • Latent. Very few if any clinical signs. • Tertiary. Gummas or granulomatous lesions develop subcutaneously, expand and ulcerate in the skin. These lesions also occur in liver, bones, other organs. Direct detection of treponemes under dark-field microscopy is diagnostic. Serologic screening tests (rapid plasma reagin (RPR) or venereal disease research laboratory (VDRL)) are reactive by day 7 of chancre and easy to perform.
TREATMENT
• In early disease, drug of choice is benzathine penicillin G, 2.4 million U i.m. once. • In late disease, drug of choice is benzathine penicillin G, 2.4 million U i.m. once a week for 3 weeks. For patients allergic to penicillin, doxycycline or tetracycline can be given. • Successful therapy indicated by falling RPR titer.






