[level-membership-for-internal-medicine-category]
Facial Swellings
Facial swelling is a common presenting complaint. It may be generalised or localised. Many cases are due to trauma or infection but it may be a sign of systemic disease.
Causes
History
Traumatic
Usually obvious history of trauma. Swelling may be severe, with bruising and closure of the palpebral fissures. Insect bites may cause swelling due to allergy or infection. The patient may not be aware of an insect bite.
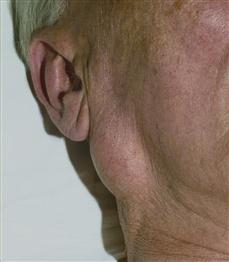
Infective
Erysipelas is an uncommon skin infection caused by streptococci. Pain and redness are apparent usually over the cheek. Pyrexia and malaise may occur. Dental infections are common (see Jaw pain and swellings, p. 262) and are often initially localised, but the side of the face may swell. There is severe associated throbbing pain. Sinusitis presents with constant unilateral pain over the frontal or maxillary sinuses. There is usually puffiness of the skin overlying the sinus. Parotitis presents with pain and swelling over the gland. If this is due to obstruction in the duct, the swelling occurs during eating, when the patient salivates, and regresses afterwards. Bilateral parotitis occurs with mumps.
Neoplastic
Neoplasia may affect the parotids, sinuses and jaw. There is usually localised swelling with carcinoma of the sinuses. The patient complains of a blocked nose and a bloodstained discharge, which may be foul-smelling. With neoplastic lesions of the jaws, there is usually deep-seated boring pain in relation to the swelling. Mediastinal tumours compress the superior vena cava and may cause suffusion of the face and facial oedema.
Vascular
Superior vena caval thrombosis may occur. This is rare and there may have been long-term central venous cannulation. There is cyanotic suffusion of the face with facial oedema. Cavernous sinus thrombosis usually presents following a history of infection of the face or in the sinuses. There may be a history of immunosuppression or diabetes. The patient complains of pain in the eye and forehead, with swelling around the eye and a protruding eye. The swelling may eventually involve the whole of the side of the face. Double vision occurs as a result of cranial nerve involvement.
Endocrine
Cushing’s syndrome presents with swelling of the face (moon face) with a typical red appearance. Facial swelling is also seen in acromegaly. The patient will usually complain of an increase in shoe size and large hands. There may also be a hoarse voice, protrusion of the jaw and cardiac failure. Congenital hypothyroidism (formerly known as cretinism) is associated with a puffy swollen face and enlargement and protrusion of the tongue. Gross acquired clinical hypothyroidism produces characteristic non-pitting oedematous changes in the skin of the face, giving rise to a characteristic clinical appearance.
Metabolic
Puffiness around the eyelids usually indicates renal failure.
Drugs
History of steroid therapy.
Other
Allergic reactions to drugs, especially antibiotics or blood transfusions may result in periorbital or facial oedema. Take a careful drug history. Angioneurotic oedema chiefly affects the eyelids and lips. Recurrent attacks of sudden onset of burning and irritation. A family history suggest the diagnosis. Paget’s disease often presents with painful enlargement of the skull, femur and clavicles and bowing of the tibia. The patient notices an increase in hat size. The forehead appears enlarged and prominent.
Examination
Traumatic
Fractures are usually obvious. Check pupillary reaction and test the cranial nerves. Insect-bite puncture wounds may be obvious but often they are not. There is often surrounding cellulitis and oedema.
Infective
Erysipelas presents as a red, tender area with well-demarcated margins raised above the surrounding normal skin. The patient is usually pyrexial. Dental abscesses are usually obvious, with local tenderness and oedema. Sinusitis is largely diagnosed from the history, with localised tenderness and swelling. With parotitis the gland is swollen and tender if infection has occurred, with occasionally redness over the skin. It may be unilateral or bilateral. Examine the orifice of the parotid duct for stone or stenosis.
Neoplastic
Neoplasia of the parotid usually presents as an enlarged, irregular, firm or hard swelling. There may have been a pre-existing pleomorphic adenoma. Test the integrity of the facial nerve, which may be affected by carcinoma. Carcinoma of the maxillary sinus may present with swelling over the sinus. Jaw swellings are considered on p. 262. Superior vena caval obstruction presents with facial oedema and cyanotic suffusion of the face. Examine the chest.
Vascular
Superior vena caval thrombosis presents in a similar way to obstruction. With cavernous sinus thrombosis, there will be oedema, redness and swelling around the orbit, spreading onto the face. Exophthalmos will be present. Test for paresis of cranial nerves III, IV and VI. The patient will usually be pyrexial and ill.
Endocrine
In Cushing’s syndrome, there will be moon face, and usually other features such as striae, buffalo hump, proximal myopathy. In congenital hypothyroidism, there is a broad, flat face, the eyes are wide apart and the tongue protrudes from the mouth. In acromegaly, there is a large face with overgrowth of the soft tissues of the face, nose, lips and tongue. The patient will have large hands and a large protuberant jaw (prognathism).
Metabolic
In renal failure, the swelling usually occurs around the eyes. There may also be peripheral oedema and hypertension. There is usually a bronze-lemon tinge to the skin in chronic renal failure.
Drugs
Steroid therapy gives an appearance similar to Cushing’s syndrome (see above).
Other
In allergic reactions, there is often swelling of the eyes, lips and face, with urticaria of other areas on the body. Laryngeal oedema and bronchospasm may occur. Angioneurotic oedema is usually diagnosed from the history. Examination will reveal swellings of the eyelids and lips, with burning and irritation. In Paget’s disease, there is an enlargement of the skull, with the vault of the skull bulging outwards above the eyes. Deafness may occur. Occasionally, there is compression of the cranial nerves. Test the cranial nerves. High output cardiac failure may be present.
General Investigations
■ FBC, ESR
Hb ↓ malignancy. WCC ↑ infection, e.g. sinusitis, cavernous sinus thrombosis. ESR ↑ infection, malignancy.
■ U&Es
Urea and creatinine ↑ in renal failure.
■ Skull X-rays
Fractures. Sinusitis – opaque sinus. Malignancy – opaque sinus and erosion of bone. Bone tumours. Paget’s disease. Pituitary fossa – acromegaly, Cushing’s disease.
■ CXR
Mediastinal tumour. Primary bronchial carcinoma with inappropriate secretion of ACTH leading to Cushing’s syndrome.
Specific Investigations
■ CT
Acromegaly. Cushing’s disease. Fractures. Mediastinal tumours. Carcinoma of the air sinuses. Parotid tumours. Cavernous sinus thrombosis.
■ Sialography
Parotid conditions, e.g. stone in parotid duct.
■ Plasma cortisol
Cushing’s syndrome.
■ Glucose tolerance test with growth hormone assay
Acromegaly.
[/level-membership-for-internal-medicine-category][not-level-membership-for-internal-medicine-category]
Facial Swellings
Facial swelling is a common presenting complaint. It may be generalised or localised. Many cases are due to trauma or infection but it may be a sign of systemic disease.
Causes
History
Traumatic
Usually obvious history of trauma. Swelling may be severe, with bruising and closure of the palpebral fissures. Insect bites may cause swelling due to allergy or infection. The patient may not be aware of an insect bite.
Infective
Erysipelas is an uncommon skin infection caused by streptococci. Pain and redness are apparent usually over the cheek. Pyrexia and malaise may occur. Dental infections are common (see Jaw pain and swellings, p. 262) and are often initially localised, but the side of the face may swell. There is severe associated throbbing pain. Sinusitis presents with constant unilateral pain over the frontal or maxillary sinuses. There is usually puffiness of the skin overlying the sinus. Parotitis presents with pain and swelling over the gland. If this is due to obstruction in the duct, the swelling occurs during eating, when the patient salivates, and regresses afterwards. Bilateral parotitis occurs with mumps.
Neoplastic
[/not-level-membership-for-internal-medicine-category]
