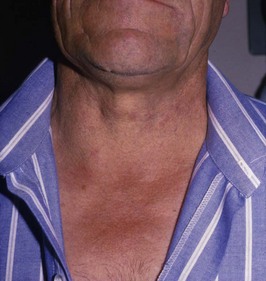
Problem 5 Swelling in the neck in a 58-year-old man
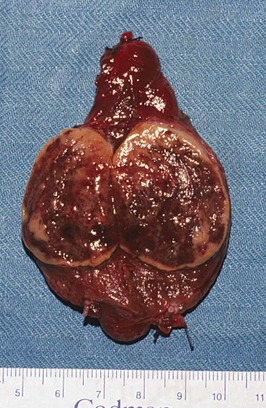
The patient undergoes a right thyroid lobectomy and makes an uneventful recovery.
Answers
A.2 You will want to know about the following:
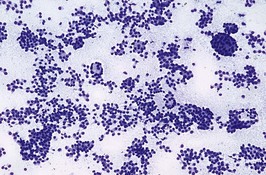
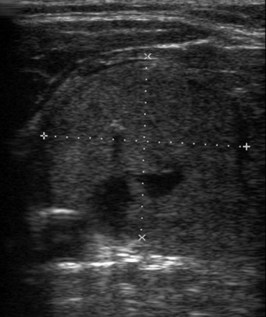
A.4 The differential diagnosis of this thyroid mass – in order of most to least common – is:
You therefore recommend to the patient the following measures:
Revision Points
Management of the Lump in the Thyroid
, www.british-thyroid-association.org. The website of the British Thyroid Association, with a number of useful links
, www.endocrinesurgeons.org.au. The website of Australian Endocrine Surgeons
, www.aace.com. The website of the American Association of Clinical Endocrinologists, with clinical guidelines for the management of thyroid carcinoma
, www.thyroidmanager.org. A site covering all aspects of thyroid disease
Yeung M.J., Serpell J.W. Management of the solitary thyroid nodule. The Oncologist. 2008;13:105-122.