Surgical Treatment of Unusual Myoma Conditions
Several bizarre variants of myoma may be encountered. Benign metastasizing myoma (leiomyomatosis peritonealis disseminata) consists of multiple intraperitoneal benign tumors and even distant myoma metastasis, typically to the lungs (Fig. 15–1). These cases may have a propensity for occurrence during pregnancy. Symptoms include paroxysmal attacks of dyspnea and hemoptysis. Myomas may regress after the pregnancy terminates (see Fig. 15–1).
Intravenous leiomyomatosis is associated with smooth muscle tumors extending into venous channels (Fig. 15–2). This condition illustrates clinically the enigma about the origins of uterine leiomyomata in general: Do these tumors arise from a smooth muscle cell from the myometrium or from a smooth muscle cell within the media of the blood vessel itself? This unusual phenomenon represents a dissociation between clinical and histologic malignancy in which benign uterine myomas may propagate via blood vascular channels, although the condition rarely kills the patient.
The uterus is typical of one containing irregularly enlarged myomata uteri (Fig. 15–3). The venous pattern over the uterus and within the broad ligament is unusually prominent, and an indurated, woody texture may be found. As the pedicles are cut, glistening, white extensions (Fig. 15–4), some as wide as 2 to 3 cm in diameter, may be seen (Fig. 15–5). As veins separate, the intravascular tumor may ooze out of the involved vessels in a wormlike fashion (Fig. 15–6). Microscopically, the vessel wall contains plugs of typical benign smooth muscle lying free within the lumen (Fig. 15–7) or attached to the wall of the vein (Fig. 15–8A, B).
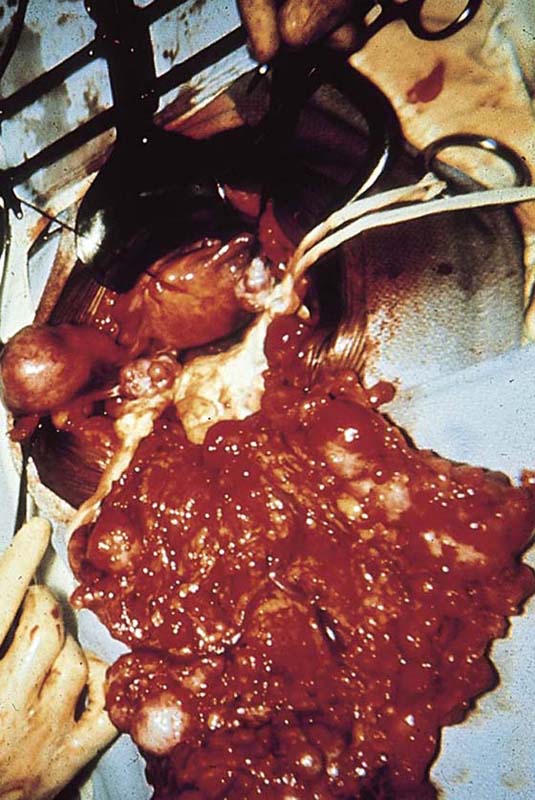
FIGURE 15–1 Leiomyomatosis peritonealis disseminata. The omentum is filled with myomata of various sizes.

FIGURE 15–2 A large intravenous myoma extension is teased out of a distended vein.

FIGURE 15–3 An enlarged irregular uterus filled with myomata. Note the submucous, intramural, subserous varieties within this single uterus.

FIGURE 15–4 A glistening white serpentine myoma is seen to enter a thin-walled venous sinus. Note that the color of the intravenous myoma is very close to the color of the surgeon’s gloves.

FIGURE 15–5 An intravenous leiomyoma extension 2 cm in diameter fills the uterine vein, giving a woody feeling to the distended uterine, parauterine, and bladder vessels.

FIGURE 15–6 As vascular pedicles are cut, the myoma oozes out of the vessels in a wormlike fashion. The differential diagnosis is between intravenous leiomyomatosis and endolymphatic stromal myosis (stromatosis).
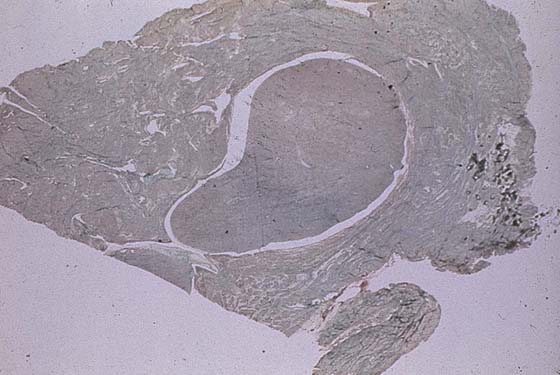
FIGURE 15–7 Elastic tissue stain shows a microscopic plug of myoma within a venous space.
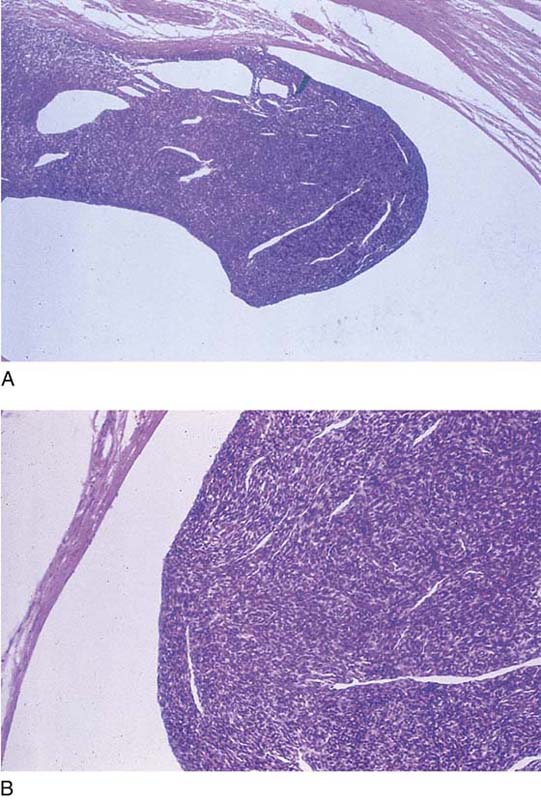
FIGURE 15–8 A. Benign myoma with a venous space and attached to the wall of the vein. B. High-power view of a benign myoma within a uterine vein.






