CHAPTER 12 Surgical Treatment of Chest Wall Deformities
Open Repair
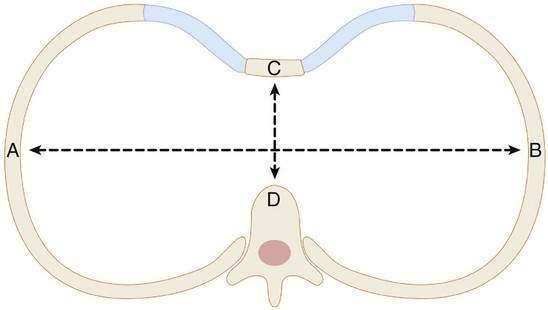
Step 1: Surgical Anatomy
Step 2: Preoperative Considerations
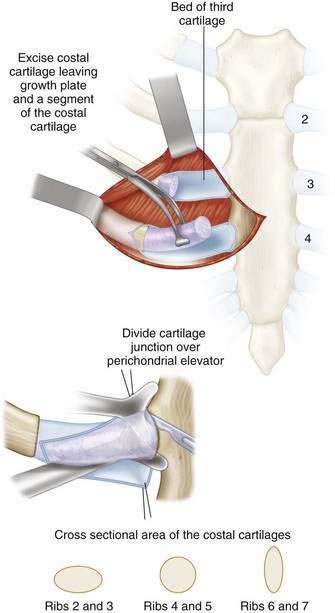
Step 3: Operative Steps
Positioning
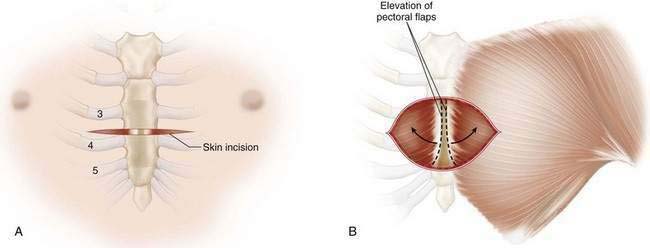
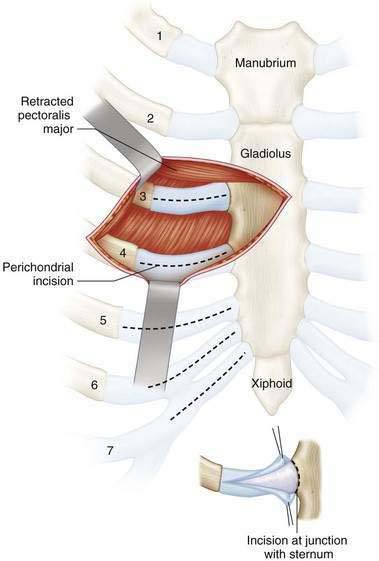
Incision
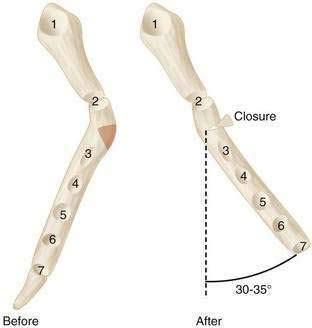
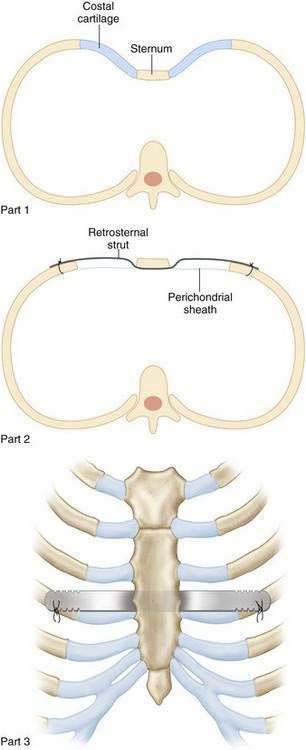
Closure
Step 4: Postoperative Care
Step 5: Pearls and Pitfalls
Aronson DC, Bosgraaf RP, Merz EM, et al. Lung function after the minimal invasive pectus excavatum repair (Nuss procedure). World J Surg. 2007;31:1518-1522.
Baronofsky ID. Technique for the correction of pectus excavatum. Surgery. 1957;42:884-890.
Beiser GD, Epstein SE, Stampfer M, et al. Impairment of cardiac function in patients with pectus excavatum, with improvement after operative correction. N Engl J Med. 1972;287:267-272.
Cahill JL, Lees GM, Robertson HT. A summary of preoperative and postoperative cardiorespiratory performance in patients undergoing pectus excavatum and carinatum repair. J Pediatr Surg. 1984;19:430-433.
Ellis DG. Experience with a variation of the transverse incision in chest wall deformity correction. J Pediatr Surg. 1997;32:728-729.
Fonkalsrud EW, Mendoza J. Open repair of pectus excavatum and carinatum deformities with minimal cartilage resection. Am J Surg. 2006;191:779-784.
Haller JAJr, Kramer SS, Lietman SA. Use of CT scans in selection of patients for pectus excavatum surgery: a preliminary report. J Pediatr Surg. 1987;22:904-906.
Kaguraoka H, Ohnuki T, Itaoka T, et al. Degree of severity of pectus excavatum and pulmonary function in preoperative and postoperative periods. J Thorac Cardiovasc Surg. 1992;104:1483-1488.
Malek MH, Berger DE, Housh TJ, et al. Cardiovascular function following surgical repair of pectus excavatum: a meta-analysis. Chest. 2006;130:506-516.
Malek MH, Fonkalsrud FW, Cooper CB. Ventilatory and cardiovascular responses to exercise in patients with pectus excavatum. Chest. 2003;124:870-882.
Shamberger RC, Welch KJ. Surgical repair of pectus excavatum. J Pediatr Surg. 1988;23:615-622.
Welch KJ. Satisfactory surgical correction of pectus excavatum deformity in childhood: a limited opportunity. J Thorac Surg. 1958;36:697-713.




