CHAPTER 26 Surgical Approach
Two surgical approaches have been described for implantation of a reverse prosthesis. The anterior superior approach was initially used because it makes use of the rotator cuff defect. More recently, the deltopectoral approach has been used for insertion of a reverse prosthesis. We perform all reverse prostheses through the deltopectoral approach, which is our preferred approach for five reasons:
TECHNIQUE FOR THE DELTOPECTORAL APPROACH
The deltopectoral approach used for implantation of a reverse prosthesis is nearly identical to the deltopectoral approach used for unconstrained shoulder arthroplasty described in Chapter 8. The skin incision, subcutaneous dissection, development of the deltopectoral interval, identification of the conjoined tendon and coracoid process, and retractor placement proceed as detailed in Chapter 8 and shown in Figures 8-1 through 8-6.
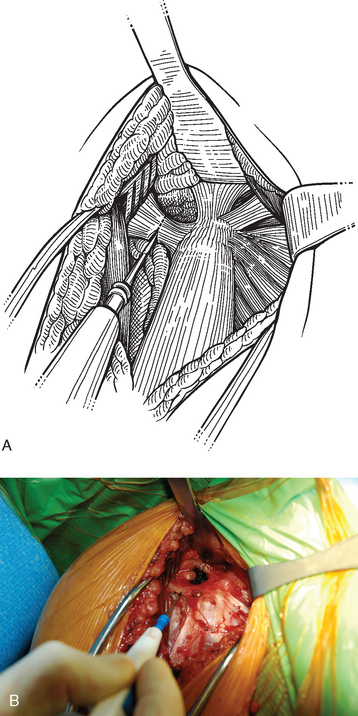
With the arm abducted and externally rotated, the apex formed by the insertion of the coracoacromial ligament and the conjoined tendon onto the coracoid process is identified. The coracoacromial ligament is sectioned just lateral to its insertion on the coracoid with a needle tip electrocautery to enhance exposure of the superiorly migrated humeral head (Fig. 26-2). This is in contrast to the surgical approach used for unconstrained shoulder arthroplasty, in which the coracoacromial ligament is preserved to act as a static restraint to anterior superior migration. When we use a reverse prosthesis, the prosthetic design eliminates the need for this static restraint.
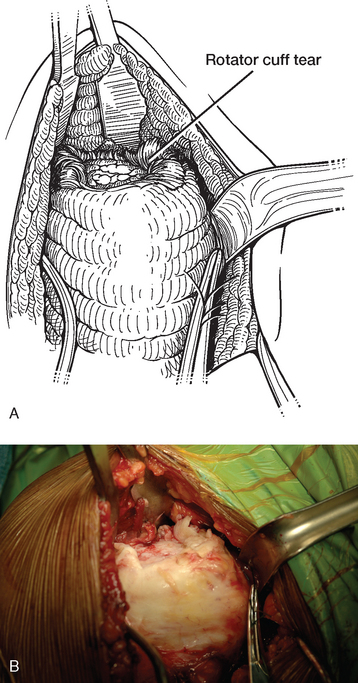
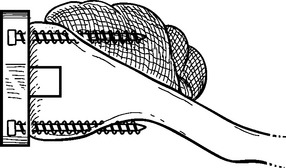
In cases in which the subscapularis is intact, it is handled identically to cases of unconstrained shoulder arthroplasty. Two stay sutures of no. 2 polyester are placed in the subscapularis tendon near the musculotendinous junction. The glenohumeral joint is often already accessible through a large rotator cuff tear superiorly (Fig. 26-3). The anatomic neck of the humerus is identified, and a scalpel is used to transect the subscapularis tendon and joint capsule along the anatomic neck of the humerus. The electrocautery replaces the scalpel at the inferior portion of the subscapularis to cauterize the previously ligated anterior humeral circumflex vessels. A humeral head retractor is placed in the glenohumeral joint and is used to retract the humeral head posteriorly. A circumferential release of the subscapularis tendon is performed, with release of the superior, middle, and inferior glenohumeral ligaments just as in unconstrained shoulder arthroplasty. The subscapularis is then tucked into the subscapularis fossa with forceps and held with a glenoid rim retractor. In contrast to cases of unconstrained arthroplasty, no sponge is placed in the subscapularis fossa because insertion of screws for fixation of the glenoid base plate risks entrapment of the sponge with screws as they penetrate the anterior scapular cortex (Fig. 26-4). If the subscapularis tendon is not present, the remaining subscapularis bursa is excised to expose the glenohumeral joint, and the humeral head retractor and glenoid rim retractor are inserted. If present, the intra-articular portion of the long head of the biceps tendon is handled as described in Chapter 5 (tenotomy or tenodesis).