CHAPTER 40 Surgery of the Breast in Poland’s Syndrome
Summary/Key Points
Poland’s Syndrome or Poland Anomaly – Introduction
These findings were published in 1841 in the Reports of Guys Hospital in London by Sir Alfred Poland who did a prosection (laboratory dissection) of an upper extremity in a patient with syndactyly.1 In 1962 a plastic surgeon named Patrick Clarkson also working in London at Guys Hospital encountered a series of three patients with hand abnormalities with accompanying breast hypoplasia. Clarkson reported these three cases2 and also found the original hand specimen that had been dissected by Poland, which had been kept in the museum of Guys Hospital.
Patient Selection
Indications
Clinical presentation
Patients with Poland’s syndrome are usually seen early in life for evaluation of upper extremity abnormalities. These are either syndactyly or synbrachydactyly and some element of upper extremity hypoplasia. A typical example of a young female patient is illustrated in Fig. 40.1.
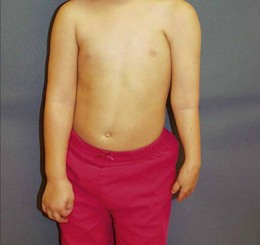
Absence of the anterolateral axillary fold is apparent during early childhood but problems with breast development may not be apparent. The potential of problems with breast development is discussed with the parents and plans are made to periodically follow patients through their young teenage years and into late adolescence (Fig. 40.2)

Alternatively, it is not uncommon for patients with breast development problems to present for the first time during the late phases of puberty for plastic surgery consultation (Fig. 40.2)
Breast Reconstruction Options – Operative Technique
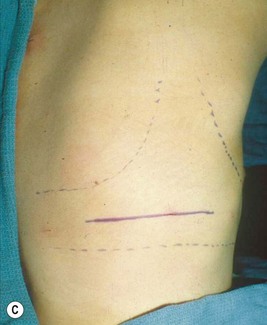
Latissimus dorsi muscle flap reconstruction
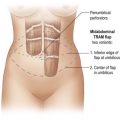
The latissimus dorsi muscle is most often available in these patients and can be used to improve the outcome of the breast reconstruction. This increases the thickness of the soft tissue envelope of the breast and either an implant or tissue expander can be placed beneath it. When the lastissmus dorsi muscle flap is transposed to the chest through a high axillary tunnel a semblance of the lateral axillary breast fold can be reconstructed. The latissimus dorsi muscle can be elevated through small incisions on the back and on the chest wall. The muscle is best transposed through a high axillary tunnel dissected in such a way as to simulate the origin of the pectoralis major muscle and the course of its lateral aspect. The muscle can be mobilized sufficiently to allow inset along the para-sternal area simulating the actual position of the sternal head of the pectoralis major muscle (see Fig. 40.5C, D). A tissue expander can be placed under the muscle to allow shaping and molding of the skin and latissimus muscle to allow the subsequent placement of an implant for completion of the breast reconstruction.
Pitfalls and How to Correct
Most reconstructions for congenital and developmental breast problems are performed with the placement of a breast implant. In my practice bilateral breast surgery is done in the majority of cases (Figs 40.3–40.5). If there is sufficient thickness of the soft tissue envelope on the side of the patient’s hypoplastic breast an implant can be placed beneath this tissue and on top of the ribs to improve breast appearance and symmetry. In cases of congenital breast deformity the goal is improvement in breast appearance not perfection. I continually reinforce this to the patient and the patient’s family. The patient pictured in Figure 40.3 had been treated in a one-stage procedure with a unilateral implant breast reconstruction as a teenager. As she matured her right breast became larger than her left and she requested a revision procedure. An implant exchange that included anterior, superior and lateral capsulotomies coupled with placing a much larger implant improved her breast appearance.












In cases where there are abnormalities in both breasts bilateral breast surgery is often needed to optimize breast appearance and symmetry. Such a case is illustrated in Fig. 40.4. This patient with Poland’s syndrome presented at age 16 with an extremely hypoplastic left breast and the ‘forme fruste’ of a constricted breast deformity on the right side. Due to the virtual absence of breast development on her left side (the affected side) and the need for considerable breast volume and dimension, reconstruction of the breast in stages was ideal. We initially achieved shaping and molding of the soft envelope of the left breast area with the preliminary placement of a tissue expander which was followed at a second stage by the placement of an implant with a contralateral mastopexy (Fig. 40.4C–F).
Postoperative Care
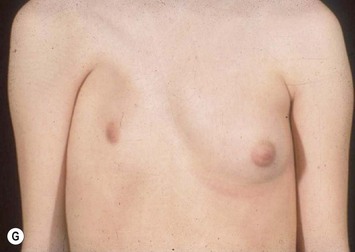
An elegant use of the latissimus dorsi for reconstruction of severe Poland’s syndrome is illustrated in Figure 40.5. This patient presented with severe breast and nipple hypoplasia and a deficiency of skin in the upper pole of the right breast with a superiorly displaced nipple–areola complex (Fig. 40.5A). In this case the quantitative deficiency of the covering soft tissue envelope was addressed first. This involved the subcutaneous placement of the expander (Fig. 40.5B) to expand the overlying breast skin thereby allowing the nipple–areola complex to be moved inferiorly. When a sufficient amount of skin had been generated, the latissimus dorsi muscle was transposed and an implant can be placed beneath the muscle to complete the reconstruction of the skin envelope, subcutaneous tissue and breast. (Fig. 40.5C, D) A breast implant was placed beneath the latissimus dorsi muscle to provide the necessary volume for a very good breast reconstruction (Fig. 40.5E–H) which was maintained at a 3-year follow up after surgery.