Surgery for Labial Hypertrophy
Michael S. Baggish  Mickey M. Karram
Mickey M. Karram
The labia minora range in size and configuration from individual to individual. These small labia play a significant anatomic role in controlling under normal circumstances ingress and egress to and from the vestibule. These labia keep the vestibular skin moist and prevent external detritus from entering the lower vagina and vestibule.
Occasionally, the labial configuration is greatly exaggerated so as to create hygienic problems (Fig. 102–1). Labial hypertrophy can also damage the tissue by snagging on clothing and tearing. Likewise, chronic irritation may create fissures and/or ulcers. For the previous circumstances, labial reduction may be indicated (Figs. 102–2 and 102–3). The procedure removes excessive tissue, leaving behind sculpted but reduced labia (Fig. 102–4). Complete amputation is rarely if ever indicated.
Other indications for labial reduction may be solely aesthetic and/or psychological. Any woman requesting labial reduction requires education about variations in vulvar anatomy and symmetry, as well as the normality of these variations. An alternative technique for simplifying excision of excess labial tissue is wedge resection, which incorporates flap advancement. The advantage of the flap advancement technique relates to the fact that the free margins of the labia minora are preserved. Therefore, the likelihood of alteration in skin color and texture is reduced. Fig. 102–5A through C schematically illustrates a Z-plasty technique. Figs. 102–6 through 102–16 show the details of a wedge-type labial plasty in a woman who desired labial reduction. The young woman complained about pulling irritation and embarrassment related to the size of her labia minora.

FIGURE 102–1 Massive hypertrophy of the labia minora in a young woman with cerebral palsy.
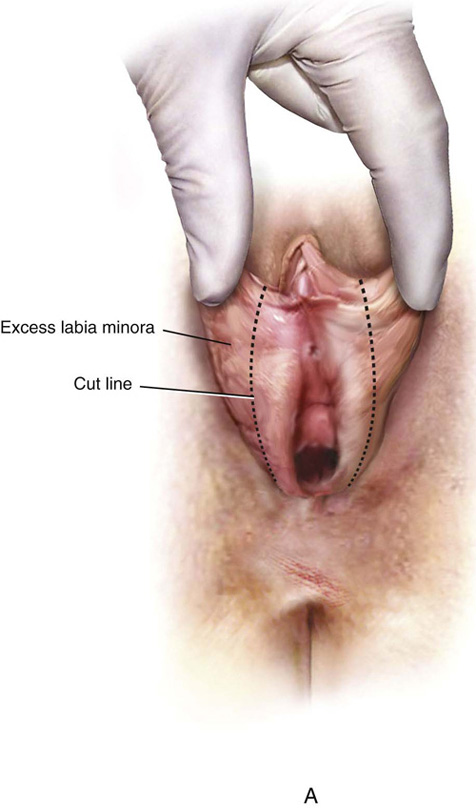
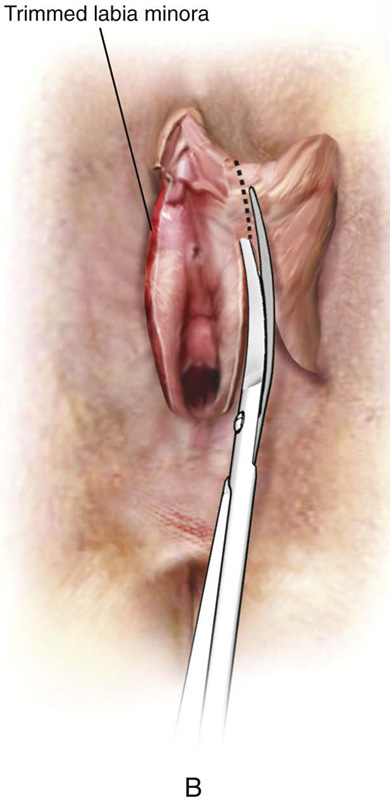

FIGURE 102–2 The technique for simple excision of enlarged or hypertrophied labial skin. A. Excess skin to be removed is marked. B. Skin is excised. C. Interrupted sutures reapproximate the edges of the labia.

FIGURE 102–3 Specimens obtained after resection of the redundant labial tissue.
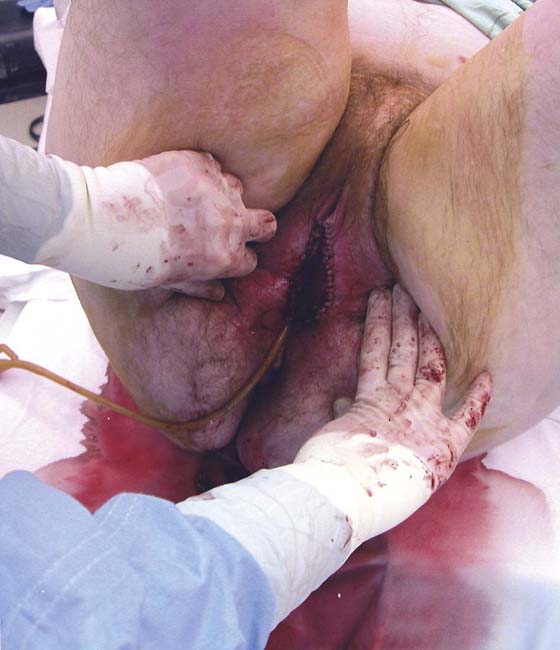
FIGURE 102–4 The repairs leave sculpted labial tissue, which will not impinge on hygiene, and maintain the appearance and function of the labia minora.
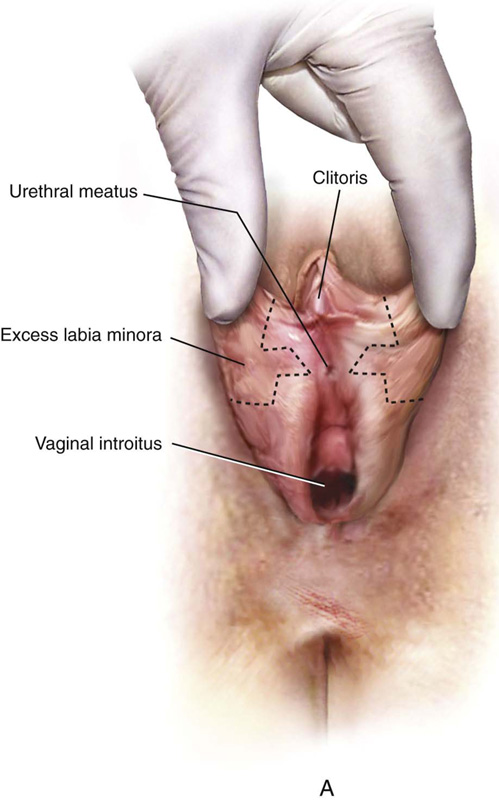
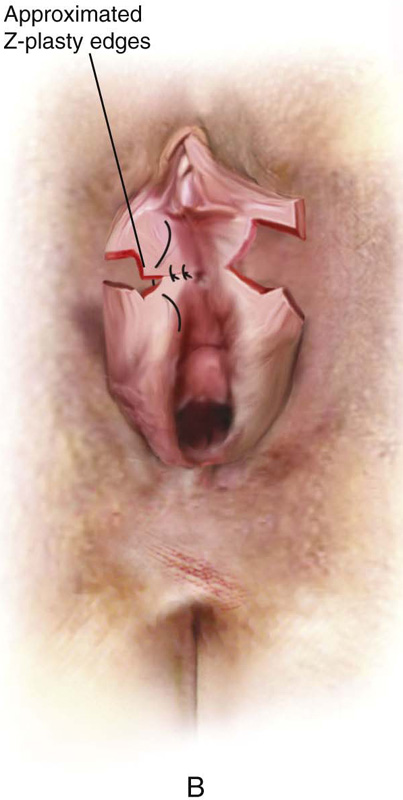

FIGURE 102–5 Technique for Z-plasty. A. Skin is to be excised. B. Skin is excised and is reapproximated transversely with fine interrupted sutures. C. Completed repair.
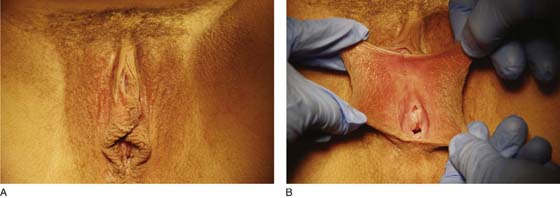
FIGURE 102–6 A. A moderate degree of labial hypertrophy is seen in this photo. B. The degree of labial enlargement is more apparent when placed on stretch.
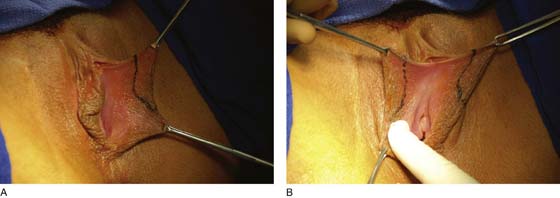
FIGURE 102–7 A. The boundaries of the wedge to be resected are marked carefully with a pen on the left labium minus. B. The wedge configuration is likewise traced on the opposite labium.

FIGURE 102–8 A 1 : 100 diluted vasopressin solution is injected into the labium for hemostasis.

FIGURE 102–9 The wedge of tissue is sharply incised on the medial aspect of the left labium minus.

FIGURE 102–10 A similar cut is made on the lateral surface of the left labium. The two cuts are connected at a precise intersection.

FIGURE 102–11 The wedge of labial tissue has been removed. The lower portion of the residual labium is mobilized upward to precisely meet the upper flap, which is marked by the application of an Allis clamp.
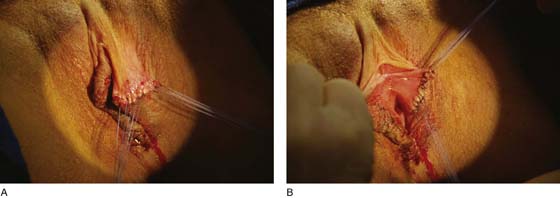
FIGURE 102–12 A. The lateral aspects of the approximated incision are sutured with 4-0 Vicryl sutures. B. The medial aspects of the wound are similarly secured.

FIGURE 102–13 Attention is now focused on the right labium minus.

FIGURE 102–14 In a fashion identical to that performed on the left side, a wedge of tissue has been excised from the right labium minus.

FIGURE 102–15 The excised wedges are shown here before they were sent to pathology.

FIGURE 102–16 The reduction is complete.






