[level-membership-for-anesthesiology-category]
49 Sural Nerve Block
The sural nerve forms from branches of the common peroneal (lateral) and tibial (medial) components of the sciatic nerve. Although the sural usually receives both contributions, anatomic variation in its composition is common.1
The sural nerve lies adjacent to the small saphenous vein within the subcutaneous tissue of the lateral leg. The sural nerve provides sensory innervation to the lateral foot.2 Because it is a sensory nerve, the sural nerve is sometimes used for biopsy or harvest. Although subcutaneous infiltration is an effective means of blocking the distal sural nerve, more proximal block may be indicated in patients with infection or edema of the foot.
Suggested Technique
Key Points
| Sural Nerve Block | The Essentials |
|---|---|
| Anatomy | The SuN emerges between the medial and lateral heads of the GC. |
| The SuN lies adjacent to the SSV within SQ tissue of the lateral leg. | |
| The SuN is about 2.5 mm in diameter. | |
| Positioning | Supine with leg elevated |
| Operator | Standing at side of patient |
| Display | Across the table |
| Transducer | High-frequency linear, 23- to 38-mm footprint |
| Initial depth setting | 20 mm |
| Needle | 25 gauge, 38 mm in length |
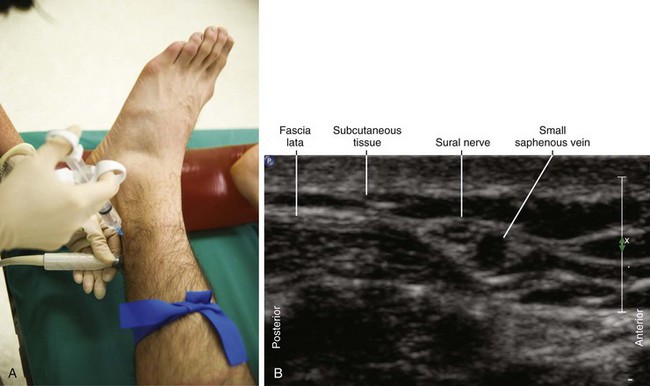
| Anatomic location | Apply a calf tourniquet to help identify the SSV. |
| Begin by scanning the lateral leg proximal to the lateral malleolus. | |
| Approach | Perform the block proximal to the lateral malleolus. |
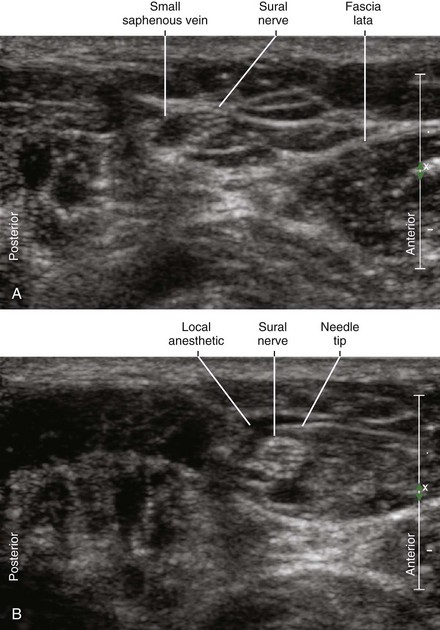
| SAX view of SuN, in-plane from anterior to posterior | |
| Sonographic assessment | The injection should track along the SuN and SSV. |
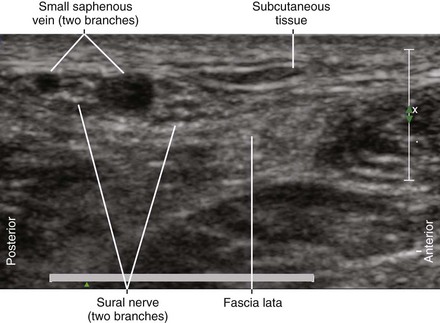
| Anatomic variation | The SuN may divide proximally. |
GC, Gastrocnemius muscle; SAX, short axis; SSV, small saphenous vein; SuN, sural nerve.
Clinical Pearls
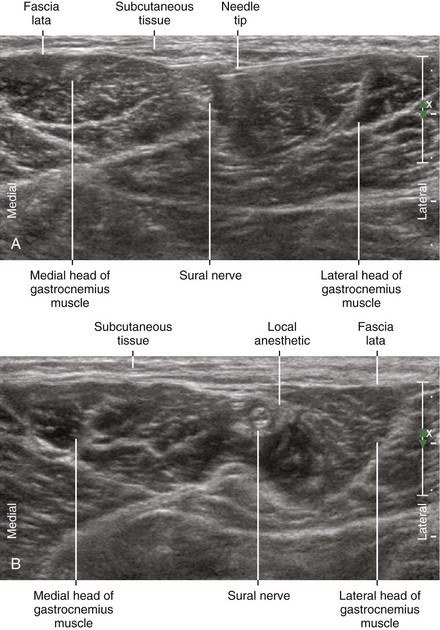
• The sural nerve emerges between the medial and lateral heads of the gastrocnemius to enter the subcutaneous tissue of the lower calf.
• In this location the sural nerve lies lateral to the small saphenous vein. When the sural nerve consists of separate branches, they typically flank either side of the small saphenous vein.1
• The sural nerve and small saphenous vein pass posterior to the lateral malleolus. Because the sural nerve lies in subcutaneous tissue in the lower calf, it is not mistaken for a nearby tendon.
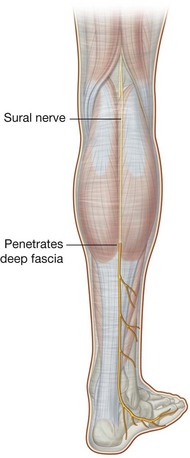
FIGURE 49-1 Course of the sural nerve.
(From Drake RL, Vogl W, Mitchell AWM. Gray’s anatomy for students. Philadelphia: Churchill Livingstone; 2004.)
1 Zhu J, Li D, Shao J, et al. An ultrasound study of anatomic variants of the sural nerve. Muscle Nerve. 2011;43(4):560–562. doi: 10.1002/mus.21918. Epub 2011, Feb 8
2 Solomon LB, Ferris L, Tedman R, et al. Surgical anatomy of the sural and superficial fibular nerves with an emphasis on the approach to the lateral malleolus. J Anat. 2001;199:717–723.
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
49 Sural Nerve Block
The sural nerve forms from branches of the common peroneal (lateral) and tibial (medial) components of the sciatic nerve. Although the sural usually receives both contributions, anatomic variation in its composition is common.1
The sural nerve lies adjacent to the small saphenous vein within the subcutaneous tissue of the lateral leg. The sural nerve provides sensory innervation to the lateral foot.2 Because it is a sensory nerve, the sural nerve is sometimes used for biopsy or harvest. Although subcutaneous infiltration is an effective means of blocking the distal sural nerve, more proximal block may be indicated in patients with infection or edema of the foot.
Suggested Technique
Key Points
| Sural Nerve Block | The Essentials |
|---|---|
| Anatomy | The SuN emerges between the medial and lateral heads of the GC. |
| The SuN lies adjacent to the SSV within SQ tissue of the lateral leg. | |
| The SuN is about 2.5 mm in diameter. |
