CHAPTER 17 Suprascapular block
Surface anatomy
The spine of the scapula is the main bony landmark for the suprascapular block (Fig. 17.1). It can be palpated from the medial aspect of the scapula and followed laterally and superiorly to the acromion. Two centimeters superior to the midpoint of the spine of the scapula is the needle insertion point.

Sonoanatomy
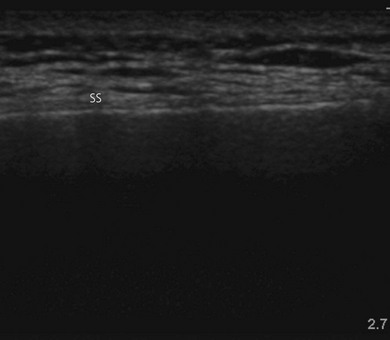
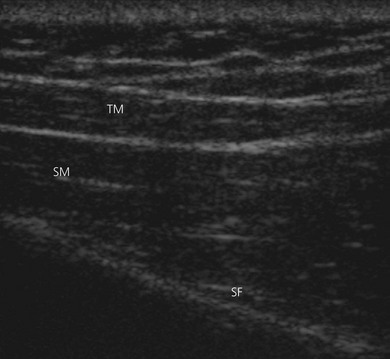
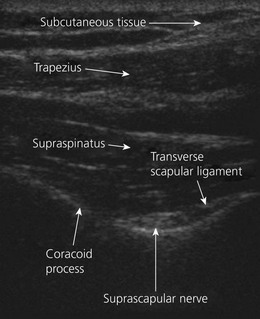
An initial scan is performed in the sagittal orientation at the superior medial border of the scapula to identify the pleura. Scanning proceeds laterally with this transducer orientation. Where the scapula moves beyond the lung field is noted. The ultrasound transducer is now placed parallel to the scapular spine (Fig. 17.2) such that the scapular spine is visualized as a superficial hyperechoic line (Fig. 17.3). By moving the transducer cephalad the suprascapular fossa is identified (Fig. 17.4). While imaging the supraspinatus muscle and the bony fossa underneath, the ultrasound transducer is slowly moved laterally (maintaining a transverse transducer orientation) to locate the suprascapular notch (Fig. 17.5). The suprascapular nerve is seen as a round hyperechoic structure at 4–6 cm depth beneath the transverse scapular ligament in the scapular notch (Fig. 17.5).

Technique
Landmark-based approach
The block is performed with the patient in the sitting or standing position, with the hand of the side to be blocked resting on the contralateral shoulder (Fig. 17.6). The operator stands behind the patient. To reduce the risk of pneumothorax, as short a needle as practical is used. Needle orientation is caudad and posterior. The needle is advanced until bony contact is made, withdrawn slightly, and 10 mL of local anesthetic injected after careful aspiration (Fig. 17.7). It is not necessary to locate the scapular notch nor to elicit paresthesia because these increase the risk of pneumothorax and nerve injury.


Ultrasound-guided approach
Intravenous access, ECG, pulse oximetry and blood pressure monitoring are established. Maximized comfort for the operator and patient is an important step in pre-procedure preparation. For the ultrasound-guided suprascapular block, the patient is placed in the sitting position. The operator stands adjacent to the side to be blocked. The ultrasound screen, transducer, needle, and plane of imaging should all be placed in one view for the operator. For the suprascapular block, the ultrasound screen is placed in front of the shoulder on the side to be blocked (Fig. 17.8). Room lights may be turned down to enhance image viewing. The operating lights can be used to maintain some working lighting in the background.

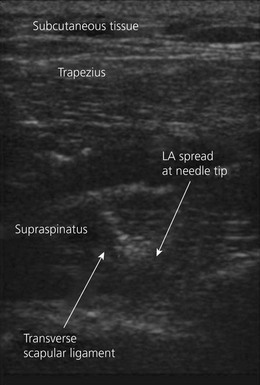
Developing and maintaining a predetermined basic scanning routine is of enormous help in improving operator confidence and success. A 21-gauge, 50-mm b-bevel needle (Stimuplex; B. Braun, Bethlehem, PA) is inserted along the longitudinal axis of the ultrasound beam (Fig. 17.9). This needle was chosen due to its good ultrasound visibility. The needle is visualized in its full course. The endpoint for injection was an ultrasound image demonstrating the needle tip in proximity to the suprascapular nerve in the suprascapular notch (Fig. 17.10). The injection and spread of local anesthetic (4–6 mL) is visualized.