Suprapubic Catheter Placement
Suprapubic catheters are commonly placed after surgeries that may delay the return of normal, efficient voiding, such as anti-incontinence procedures and procedures for pelvic organ prolapse. Suprapubic catheters are thought to improve patient comfort and ease of nursing care; however, the real advantage is that they allow patients to control voiding trials, thus obviating repeated transurethral catheterizations to check postvoid residual volumes.
The major catheter types available are listed in Table 87–1 and shown in Fig. 87–1. Suprapubic catheters can be inserted using an open or a closed technique. Open techniques are commonly utilized at the time of abdominal surgeries, such as a retropubic urethropexy. Any of the catheter types listed in Table 87–1, as well as a Foley catheter, can be used. To perform the open technique of suprapubic catheter placement, the bladder is filled in a retrograde fashion with saline or water, usually through a three-way Foley catheter. A stab incision is made through the skin above or below a transverse skin incision or off to one side of the lower end of a vertical incision. If a Foley catheter is going to be used, a curved clamp is passed from the undersurface of the rectus muscle and fascia and then out the stab wound (Fig. 87–2A). The Foley catheter is then pulled into the field and is brought into close proximity to the extraperitoneal portion of the dome of the bladder (Fig. 87–2B). If a high extraperitoneal cystotomy has already been made to assess bladder integrity or ureteral patency, the Foley catheter is placed into the same incision of the bladder and the cystotomy is closed in two layers around the catheter (Fig. 87–3) (see description of opening and closing the bladder in Chapter 88). If suprapubic teloscopy has been performed (see Chapter 123), the catheter is placed through the same stab wound in which teloscopy is performed (Fig. 87–4). Otherwise, a stab wound is placed in the extraperitoneal dome of the bladder, the catheter is placed directly into the bladder, and a purse string suture is placed and tied around the catheter (Fig. 87–5). If a commercially available suprapubic catheter is used, the catheter and an introducer are placed into the previously made stab wound in the skin and inserted through the skin muscle and fascia. The bladder is then punctured through the dome, taking care to avoid large vessels. The catheter is advanced through the sheath or over the needle guide, which is simultaneously withdrawn. Efflux of urine or saline should be ensured. If the catheter has a balloon, it is inflated and the catheter is sutured in place on the skin.
Closed insertion can be performed using a variety of catheters (see Table 87–1 and Figure 87–1) and is commonly done after vaginal procedures. The patient should be placed in a Trendelenburg’s position and the bladder filled with at least 500 mL of sterile water or until the bladder is easily palpable abdominally. This positioning helps ensure that no bowel lies between the bladder and the anterior abdominal wall. After the usual skin prepping, the needle or trocar should be inserted through the skin and fascia and into the bladder at a point no more than 3 cm above the pubic symphysis. The trocar or needle is removed (peeled away) and the catheter secured (Fig. 87–6). The transurethral catheter can then be removed.
A third method of suprapubic insertion of a Foley or Malecot catheter is to insert a perforated urethral sound or Lowsley retractor transurethrally into the bladder. The tip of the sound is directed anteriorly into the bladder dome, and the abdominal wall is tented upward by the sound (Fig. 87–7). A suprapubic stab wound is made into the bladder right over the sound or retractor. The catheter is sutured to the sound in the suprapubic area and pulled backward through the bladder and out the external urethral meatus, where the suture is removed. The catheter is then withdrawn into the bladder and the balloon is inflated. This technique allows placement of very large Foley catheters (22F) to be used as suprapubic tubes.
TABLE 87–1  Types of Suprapubic and Self-Catheterization Catheters
Types of Suprapubic and Self-Catheterization Catheters
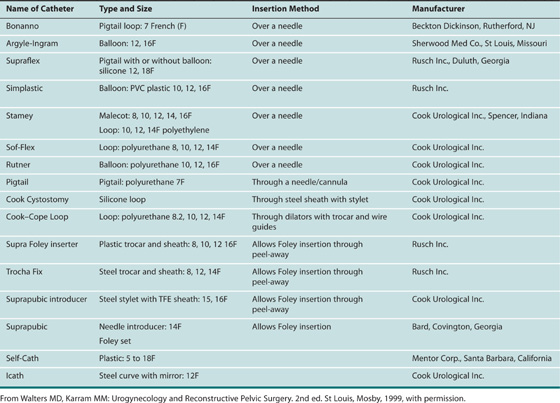
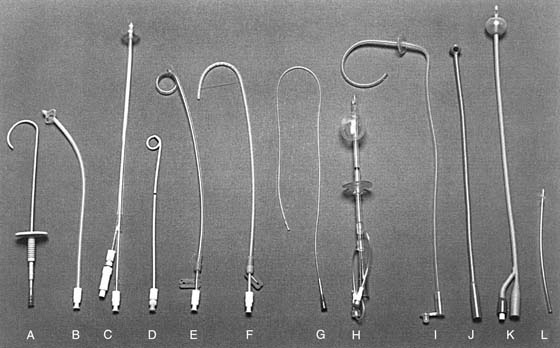
FIGURE 87–1 Suprapubic and self-catheterization bladder drainage catheters. A. Bonanno, 7 French (F). B. Stamey Malecot, 12 or 14F. C. Rutner balloon, 16F. D. Pigtail, 7F. E. Sof-Flex loop, 14F. F. Stamey loop, 12F. G. Cystocath, 8F. H. Argyle-Ingram, 12 or 16F. I. Robertson, 15F. J. Malecot. K. Foley. L. Mentor Self-Cath, 14F. (From Walters MD, Karram MM: In Urogynecology and Reconstructive Pelvic Surgery, 2nd ed. St Louis, Mosby, 1999, with permission.)
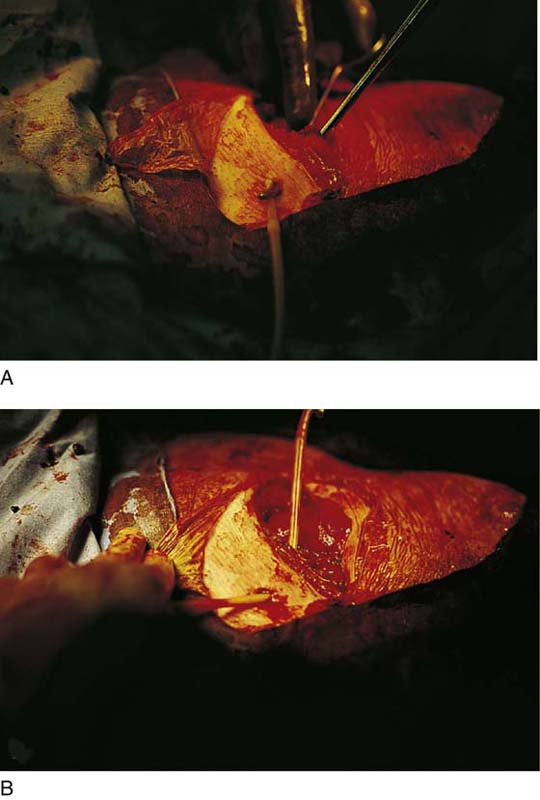
FIGURE 87–2 The Foley catheter to be used as a suprapubic catheter is being brought through a separate skin incision at the time of abdominal surgery. A. A Kelly clamp is passed through a stab wound below the incision, and the catheter is grasped. B. The catheter is pulled through the stab wound.

FIGURE 87–3 The Foley catheter has been placed through an extraperitoneal cystotomy. Note that the bladder has been closed around the catheter in two layers.

FIGURE 87–4 Suprapubic teloscopy is being performed. Note that a purse string suture has been placed through the muscular portion of the bladder wall.

FIGURE 87–5 The Foley catheter has been passed through a stab wound in the dome of the bladder. The purse string suture is tied and cut.
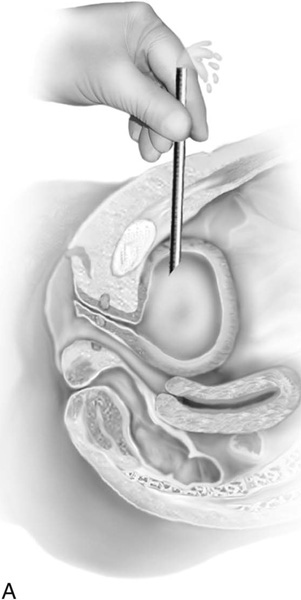
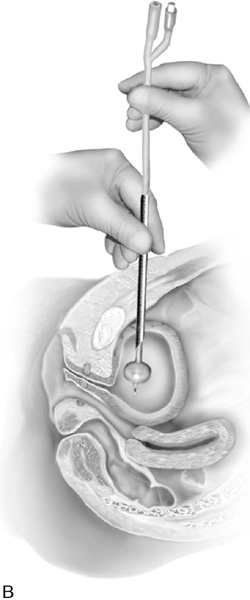
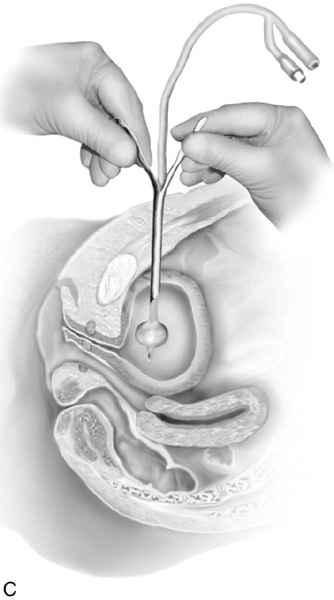
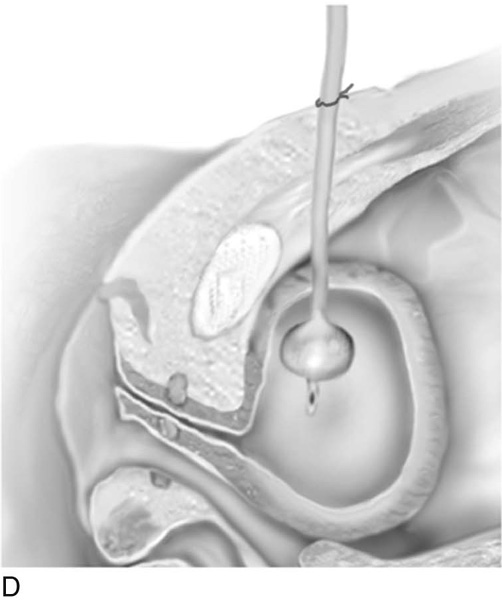
FIGURE 87–6 Technique of closed insertion of a suprapubic catheter. A. With the patient in Trendelenburg’s position, a stab incision in the skin is made approximately 3 cm above the symphysis. The trocar or the suprapubic tube is passed into the bladder, and efflux of urine is noted. B. A Foley catheter is passed down the trocar into the bladder, and the 5-mL balloon is inflated. C. The peel-away sheath is removed, and (D) the Foley catheter is fixed to the skin with a permanent suture placed in a purse string fashion.
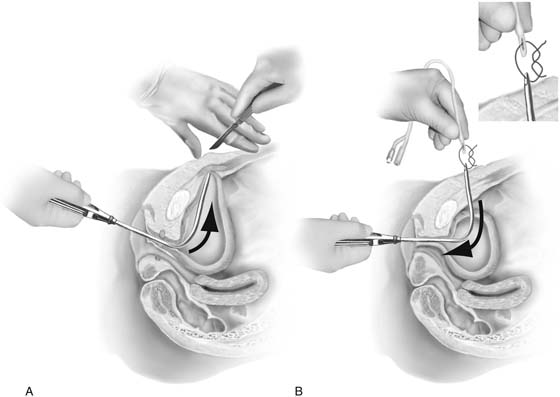
FIGURE 87–7 Alternative method of insertion of a suprapubic catheter using a transurethral sound. A. Tenting of the anterior abdominal wall with a uterine sound in preparation for a suprapubic incision. B. The catheter is pulled into the bladder. The inset demonstrates the temporary suture used to secure the Foley catheter to the tip of the sound. This technique allows placement of very large Foley catheters to be used as suprapubic tubes.






