48 Superficial Peroneal Nerve Block
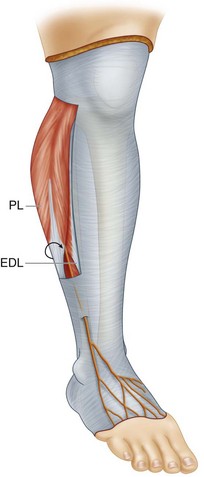
The superficial peroneal nerve is a branch of the common peroneal nerve that emerges from the neck of the fibula between the extensor digitorum longus and peroneal muscles to enter the subcutaneous tissue of the lateral leg. When emerging from the fibular neck, the superficial peroneal nerve most commonly lies in the lateral compartment of the leg. The superficial peroneal nerve ascends along the anterior intermuscular septum to pierce the fascia lata at the juncture of the middle and lower thirds of the leg. The nerve usually divides into its medial and lateral branches once in the subcutaneous tissue.1,2
Some elect to infiltrate local anesthetic over the dorsum of the foot for superficial peroneal nerve block and reserve ultrasound for the deeper nerves of the ankle block.3 However, superficial peroneal nerve block in the leg can be useful when edema or infection contraindicates more distal ankle block. Proximal ultrasound-guided superficial peroneal nerve block (along with sural block) can provide surgical anesthesia for hardware removal from the lateral ankle in weight-bearing patients. In addition, ultrasound-guided superficial block in the leg is less painful than subcutaneous infiltration across the dorsum of the foot for more distal block and does not pierce the extensor tendons of the foot.
Suggested Technique
Key Points
| Superficial Peroneal Nerve Block | The Essentials |
|---|---|
| Anatomy | The SPN emerges between the EDL and PL along the intermuscular septum. |
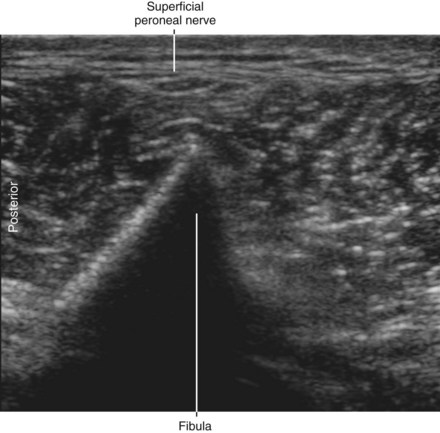
| The fibular ridge points to the SPN. | |
| The fibular artery often lies adjacent to the SPN (zoom). | |
| Positioning | Supine |
| Operator | Standing on the side of the patient |
| Display | Across the table |
| Transducer | High-frequency linear, 23- to 38-mm footprint |
| Initial depth setting | 20 mm |
| Needle | 25 gauge, 38 mm in length |
| Anatomic location | Begin imaging the lateral leg 10 cm proximal to the malleolus. |
| This is where the SPN pierces the FL. | |
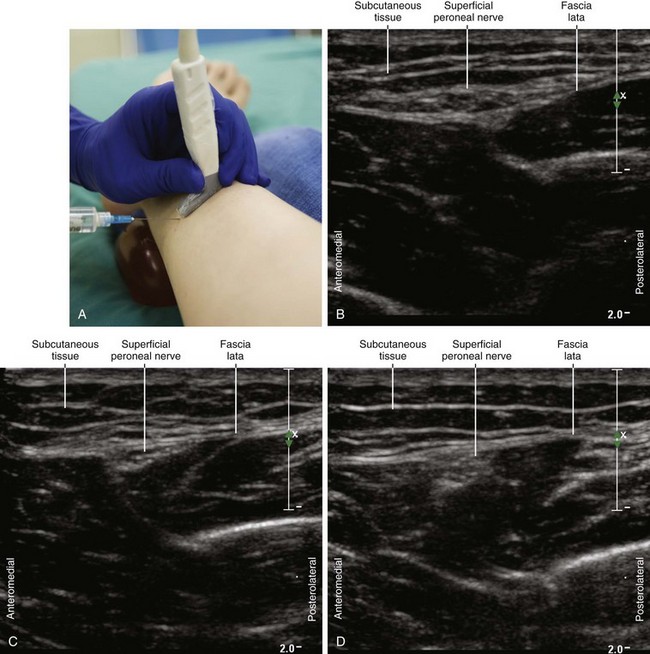
| Approach | SAX view of SPN, in-plane either direction |
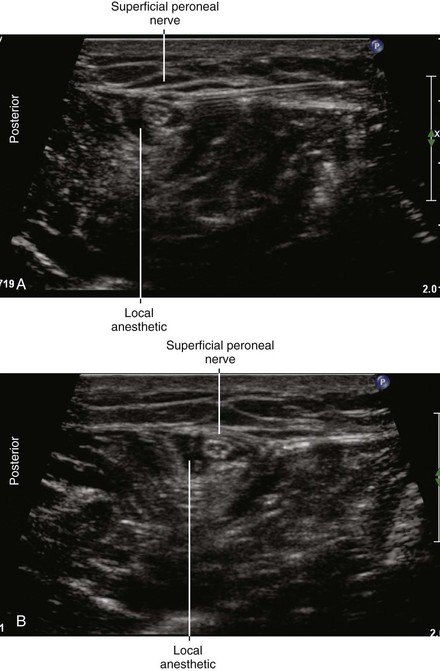
| Place the needle tip between the FL and SPN. | |
| Sonographic assessment | The injection should track proximally and descend along with the SPN. |
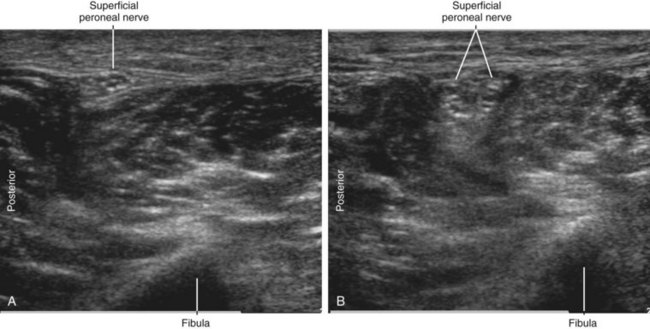
| Anatomic variation | The SPN can divide proximally in the leg. |
Clinical Pearls
• Begin by scanning anterior and proximal to the lateral malleolus with the probe perpendicular to the known course of the superficial peroneal nerve.
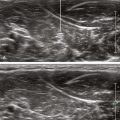
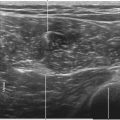
• The superficial peroneal nerve emerges in the groove between the extensor digitorum longus and peroneal muscles. The nerve is most visible where it emerges to lie against the fascia lata (10 to 16 cm proximal to the lateral malleolus, 7 cm posterolateral to the tibial crest).
• When the superficial peroneal nerve is divided by the intermuscular septum, it continues distally as the medial and intermediate dorsal cutaneous nerves of the foot.
• When two adjacent nerves are identified within the field of view, confirm that they join proximally.
• The diameters of the superficial peroneal nerve and its branches are approximately 3 and 2 mm, respectively. The superficial peroneal nerve is often accompanied by a small fibular artery and vein.
• Conditions that contraindicate ankle block (e.g., edema and infection) are not common in outpatients. Popliteal blocks are much more commonly used than more distal blocks in these settings because patient disposition is not an issue.
1 Canella C, Demondion X, Guillin R, et al. Anatomic study of the superficial peroneal nerve using sonography. AJR Am J Roentgenol. 2009;193(1):174–179.
2 Solomon LB, Ferris L, Tedman R, et al. Surgical anatomy of the sural and superficial fibular nerves with an emphasis on the approach to the lateral malleolus. J Anat. 2001;199:717–723.
3 Chin KJ, Wong NW, Macfarlane AJ, et al. Ultrasound-guided versus anatomic landmark-guided ankle blocks: a 6-year retrospective review. Reg Anesth Pain Med. 2011;36(6):611–618.