Subfertility
Endocrine investigations in the subfertile woman
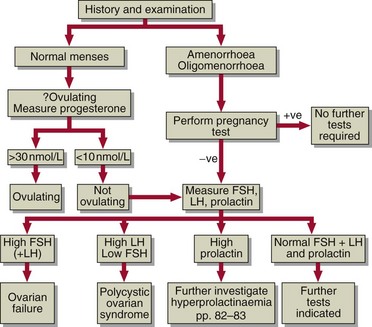
In women who present with irregular or absent menstruation (oligomenorrhoea or amenorrhoea) or who are not ovulating, hormone measurements may be diagnostic. A protocol for investigation is shown in Figure 51.1. Measurement of oestradiol and gonadotrophin concentrations may detect primary ovarian failure or polycystic ovarian disease. Measurement of prolactin, and androgens, may also assist.






Endocrine investigations in the subfertile man
In the eugonadal male with normal sperm analysis, no endocrine investigations are required. In the hypogonadal male, testosterone and the gonadotrophins should be measured first (Fig 51.2). Causes of subfertility in the male include:
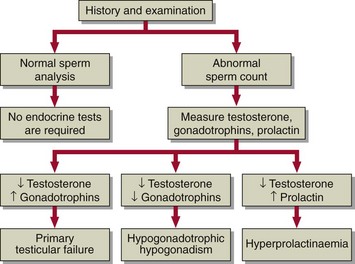
 Primary testicular failure. Where both the interstitial cells and tubules are damaged, FSH and LH will be elevated and testosterone reduced. Where tubular function only is impaired, FSH is selectively increased and androgen levels may be normal.
Primary testicular failure. Where both the interstitial cells and tubules are damaged, FSH and LH will be elevated and testosterone reduced. Where tubular function only is impaired, FSH is selectively increased and androgen levels may be normal.

 Hyperprolactinaemia. This is a rare cause of subfertility in the male (pp. 84–85).
Hyperprolactinaemia. This is a rare cause of subfertility in the male (pp. 84–85).




