[level-membership-for-cardiovascular-category]
CHAPTER 96 Subclavian Steal Syndrome
The aortic arch extends from approximately the level of the upper border of the second sternocostal articulation on the right, runs superiorly, posteriorly, and to the left in front of the trachea, where it then turns posteriorly left of the trachea and finally inferiorly on the left side of the body. The branches that conventionally arise from the arch are the right brachiocephalic artery, the left common carotid artery, and the left subclavian artery (see Chapter 71).
DEFINITION
Subclavian steal syndrome is defined as stenosis or occlusion of the subclavian artery proximal to the origin of the vertebral artery, with consequent reversal of blood flow in the vertebral artery to supply the distal subclavian artery, resulting in neurologic symptoms. This reversal of flow is said to “steal” blood from the intracranial circulation, which can cause ischemia or stroke.1 In the absence of neurologic symptoms, the constellation of findings can be called subclavian steal phenomenon.
ETIOLOGY AND PATHOPHYSIOLOGY
Atherosclerosis is the most common cause of subclavian steal syndrome. Although Takayasu arteritis is an infrequent cause of the syndrome, it occurs more commonly in people of Asian descent.2
Vollmar and colleagues3 have described four categories of subclavian steal phenomenon based on the vascular territories that provide and receive flow—vertebrovertebral, carotid-basilar, external carotid-vertebral, and carotid-subclavian. Another classification scheme4 is based on the degree of hemodynamic disturbances of the vertebral artery: stage I (occult steal, decreased blood flow), stage II (partial steal, transient or partial reversal of flow), and stage III (complete steal, permanent reversal of flow).
When the collateral flow directs a large amount of flow into the subclavian artery and away from the brain, neurologic symptoms can occur. Such symptoms have been reported to occur in approximately 36% of patients.5 Often, the circle of Willis can provide enough collateral circulation to the brainstem to avert neurologic symptoms. If the posterior communicating artery is stenotic, occluded, or absent, or if there is concomitant carotid disease, then neurologic symptoms are more likely to occur.
MANIFESTATIONS OF DISEASE
Clinical Presentation
Most patients with reversal of flow in the vertebral artery have neurologic symptoms.5 In the absence of neurologic symptoms, patients are said to have subclavian steal phenomenon.
Neurologic symptoms of subclavian steal syndrome include lightheadedness, dizziness, vertigo, upper extremity numbness, visual alterations, transient ischemic attacks and, rarely, seizures or stroke.6–8 Ipsilateral upper extremity exercise increases the blood flow demand in the subclavian artery and can cause transient neurologic symptoms caused by an increase in diversion of intracranial blood flow.9
On physical examination, subclavian steal may manifest with a subclavian artery bruit or reduced blood pressure in the ipsilateral upper extremity, along with weakness of the radial pulse.10
Imaging Techniques and Findings
Ultrasound
Sonography is the initial imaging examination when subclavian steal syndrome is suspected. Ultrasound with pulsed Doppler spectral analysis can demonstrate patency and flow direction in the vertebral artery and can establish the presence of subclavian steal.11,12
Subclavian steal phenomenon is associated with specific vertebral artery waveforms. There are four types of waveforms that indicate the degree of abnormal hemodynamics11:
In occult steal (Branchereau stage I),4 the pulsed wave Doppler spectrum typically demonstrates antegrade vertebral flow with midsystolic deceleration.11,12 The waveform may show a reversed late systolic flow as a response to reactive hyperemia in the upper extremity after arm exercise (see Fig. 96-1B). In partial subclavian steal (stage II), pulsed wave Doppler depicts partial flow reversal. The Doppler waveform in occult and partial subclavian steal has been described as the bunny rabbit sign because of its resemblance to the outline of a rabbit (Fig. 96-1A).11,12
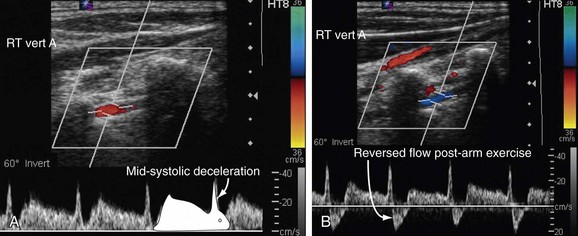
 FIGURE 96-1
FIGURE 96-1In complete (stage III) subclavian steal, the pulsed wave Doppler spectrum shows complete reversal of flow in the vertebral artery (Fig. 96-2).12
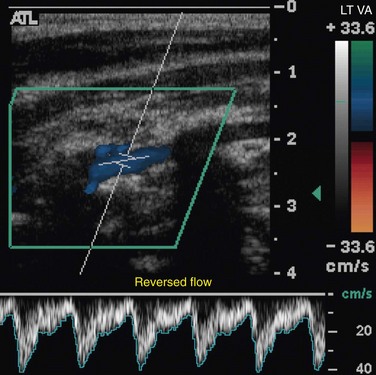
 FIGURE 96-2
FIGURE 96-2Recently, transcranial Doppler ultrasound has been studied for evaluation of flow reversal in the basilar artery in the presence of retrograde vertebral artery flow.13 Transcranial Doppler ultrasonography can be used to determine if there is reversal of basilar artery flow, which occurs in fewer than 25% of patients with retrograde vertebral flow. This is especially useful before intervention in patients with neurologic symptoms.
Computed Tomography
Contrast-enhanced computed tomography (CT) can demonstrate subclavian artery stenosis or occlusion with patency of the ipsilateral vertebral artery (Fig. 96-3).14 The obstructive lesion is often associated with calcification. Coronal reformations are often useful to depict the site of narrowing. CT can also be used to identify indirect signs of subclavian steal phenomenon, such as poor internal mammary opacification or decreased unilateral brain perfusion.15,16
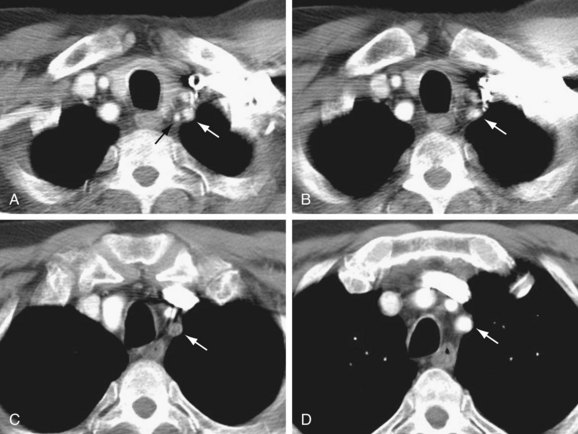
 FIGURE 96-3
FIGURE 96-3Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) can accurately and noninvasively depict the features of subclavian steal phenomenon.17 Contrast-enhanced magnetic resonance angiography (MRA) or noncontrast MRA can reveal the site of stenosis or occlusion (Figs. 96-4 and 96-5).18 Time-resolved three-dimensional MRA has been described as a means of identifying reversal of vertebral artery flow.19,20 Time-of-flight MRA has also been used to evaluate vertebral flow direction, but this technique may be less reliable (Fig. 96-6).18 Phase contrast MRI can confirm the reversal of blood flow in the vertebral artery, and velocity-encoded cine phase contrast MRI can be used to quantify velocity and flow in the vertebral and subclavian arteries (Fig. 96-7).21 The carotid and vertebral arteries, and even the circle of Willis, can be evaluated in the same examination.

 FIGURE 96-4
FIGURE 96-4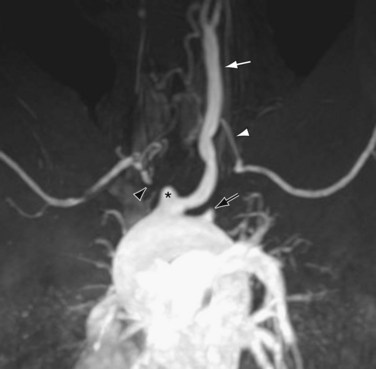
 FIGURE 96-5
FIGURE 96-5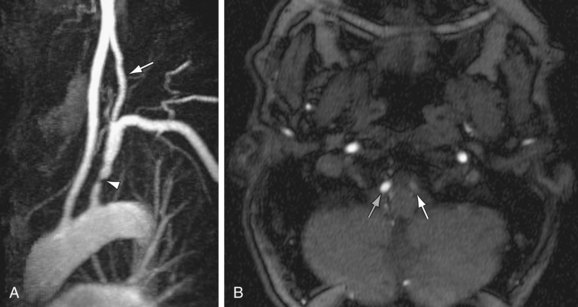
 FIGURE 96-6
FIGURE 96-6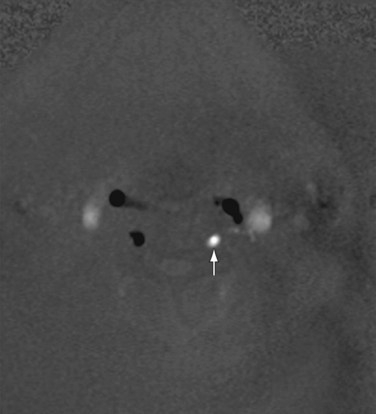
 FIGURE 96-7
FIGURE 96-7Angiography
Angiography can show stenotic or occlusive lesions in the subclavian, carotid, and vertebral arteries, as well as reversal of flow in the vertebral artery (Fig. 96-8). The use of angiography is limited by the widespread availability of ultrasound, CT, and MRI, but angiography does play an important role in the guidance of endovascular therapy.
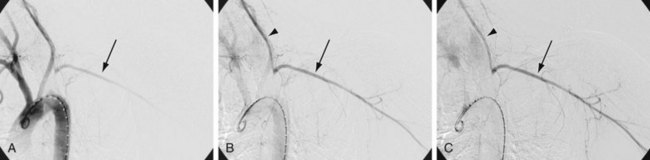
 FIGURE 96-8
FIGURE 96-8SYNOPSIS OF TREATMENT OPTIONS
Surgical and Interventional Therapy
Percutaneous intervention is indicated when reversal of vertebral blood flow is detected in a symptomatic patient. Angioplasty and stenting of the subclavian artery are performed with the goal of improving blood flow to the upper extremity, thereby reverting to antegrade vertebral flow and improving intracranial blood flow.22
If the lesion is not amenable to endovascular intervention, surgery can be performed. Surgical options include carotid-subclavian bypass, axilloaxillary bypass, and carotid-subclavian transposition.23,24 It is important to perform revascularization of a coexisting hemodynamically significant carotid artery.





Gosselin Gosselin C, Walker PM. Subclavian steal syndrome: existence, clinical features, diagnosis and management. Semin Vasc Surg. 1996;9:93-97.
Bitar Bitar R, Gladstone D, Sahlas D, Moody A. MR Angiography of subclavian steal syndrome: pitfalls and solutions. AJR Am J Roentgenol. 2004;183:1840-1841.
1 Reivich M, Holling HE, Roberts B, Toole JF. Reversal of blood flow through the vertebral artery and its effect on cerebral circulation. N Engl J Med. 1961;265:878-885.
2 Roldan-Valadez E, Hernandez-Martinez P, Osorio-Peralta S, et al. Imaging diagnosis of subclavian steal syndrome secondary to Takeyasu arteritis affecting a left-side subclavian artery. Arch Med Res. 2003;34:433-438.
3 Vollmar J, Elbayar M, Kolmar D, et al. Cerebral circulatory insufficiency in occlusive processes of the subclavian artery (“subclavian steal effect”). Dtsch Med Wochenschr. 1965;90:8-14.
4 Branchereau A, Magnan PE, Espinoza H, Bartoli JM. Subclavian artery stenosis: hemodynamic aspects and surgical outcome. J Cardiovasc Surg. 1991;32:604-612.
5 Hennerici M, Klemm C, Rautenberg W. The subclavian steal phenomenon: a common vascular disorder with rare neurologic deficits. Neurology. 1988;38:669-673.
6 Fields WS, Lemak NA. Joint study of extracranial arterial occlusion. VII. Subclavian steal—a review of 168 cases. JAMA. 1972;222:1139-1143.
7 Bornstein NM, Norris JW. Subclavian steal: a harmless haemodynamic phenomenon? Lancet. 1986;2:303-305.
8 Ioannides MA, Eftychiou C, Georgiou GM, Nicolaides E. Takayasu arteritis presenting as epileptic seizures: a case report and brief review of the literature. Rheumatol Int. 2009;29:703-705.
9 Kaneko K, Fujimoto S, Okada Y, et al. SPECT evaluation of cerebral blood flow during arm exercise in patients with subclavian steal. Ann Nucl Med. 2007;21:463-470.
10 Gosselin C, Walker PM. Subclavian steal syndrome: existence, clinical features, diagnosis and management. Semin Vasc Surg. 1996;9:93-97.
11 Kliewer MA, Hertzberg BS, Kim DH, et al. Vertebral artery Doppler waveform changes indicating subclavian steal physiology. AJR Am J Roentgenol. 2000;174:815-819.
12 Tahmasebpour HR, Buckley AR, Cooperberg PL, Fix CH. Sonographic examination of the carotid arteries. Radiographics. 2005;25:1561-1575.
13 Harper C, Cardullo PA, Weyman AK, Patterson RB. Transcranial Doppler ultrasonography of the basilar artery in patients with retrograde vertebral artery flow. J Vasc Surg. 2008;48:859-864.
14 Park JH, Chung JW, Lee KW, et al. CT angiography of Takayasu arteritis: comparison with conventional angiography. J Vasc Interv Radiol. 1997;8:393-400.
15 Alegret RE, Blandon RJ, Kirsch J. Poor left internal mammary artery opacification on coronary CT angiography: an indirect sign of subclavian steal. J Vasc Interv Radiol. 2008;19:1791-1792.
16 Huang BY, Castillo M. Radiological reasoning: extracranial causes of unilateral decreased brain perfusion. AJR Am J Roentgenol. 2007;189(6 Suppl):S49-S54.
17 Van Grimberge F, Dymarkowski S, Budts W, Bogaert J. Role of magnetic resonance in the diagnosis of subclavian steal syndrome. J Magn Reson Imaging. 2000;12:339-342.
18 Bitar R, Gladstone D, Sahlas D, Moody A. MR Angiography of subclavian steal syndrome: pitfalls and solutions. AJR Am J Roentgenol. 2004;183:1840-1841.
19 Schubert R. Time-resolved, contrast-enhanced 3D MR angiography in the subclavian steal effect. Vasa. 2010;39:85-93.
20 Virmani R, Carroll R, Hung J, et al. Diagnosis of subclavian steal syndrome using dynamic time-resolved magnetic resonance angiography: a technical note. Magn Reson Imaging. 2008;26:287-292.
21 Bauer AM, Amin-Hanjani S, Alaraj A, Charbel FT. Quantitative magnetic resonance angiography in the evaluation of the subclavian steal syndrome: report of 5 patients. J Neuroimaging. 2009;19:250-252.
22 Rodriguez-Lopez JA, Werner A, Martinez R, et al. Stenting for atherosclerotic occlusive disease of the subclavian artery. Ann Vasc Surg. 1999;13:254-260.
23 Stipa S, Cavallaro A, Sciacca V, et al. Cross-over axillary by-pass. Treatment of subclavian or innominate artery obstructive lesions. Int Angiol. 1987;6:421-427.
24 Deriu GP, Milite D, Verlato F, et al. Surgical treatment of atherosclerotic lesions of subclavian artery: carotid-subclavian bypass versus subclavian-carotid transposition. J Cardiovasc Surg. 1998;39:729-734.
[/level-membership-for-cardiovascular-category][not-level-membership-for-cardiovascular-category]
CHAPTER 96 Subclavian Steal Syndrome
The aortic arch extends from approximately the level of the upper border of the second sternocostal articulation on the right, runs superiorly, posteriorly, and to the left in front of the trachea, where it then turns posteriorly left of the trachea and finally inferiorly on the left side of the body. The branches that conventionally arise from the arch are the right brachiocephalic artery, the left common carotid artery, and the left subclavian artery (see Chapter 71).
DEFINITION
Subclavian steal syndrome is defined as stenosis or occlusion of the subclavian artery proximal to the origin of the vertebral artery, with consequent reversal of blood flow in the vertebral artery to supply the distal subclavian artery, resulting in neurologic symptoms. This reversal of flow is said to “steal” blood from the intracranial circulation, which can cause ischemia or stroke.1 In the absence of neurologic symptoms, the constellation of findings can be called subclavian steal phenomenon.
ETIOLOGY AND PATHOPHYSIOLOGY
Atherosclerosis is the most common cause of subclavian steal syndrome. Although Takayasu arteritis is an infrequent cause of the syndrome, it occurs more commonly in people of Asian descent.2
Vollmar and colleagues3 have described four categories of subclavian steal phenomenon based on the vascular territories that provide and receive flow—vertebrovertebral, carotid-basilar, external carotid-vertebral, and carotid-subclavian. Another classification scheme4 is based on the degree of hemodynamic disturbances of the vertebral artery: stage I (occult steal, decreased blood flow), stage II (partial steal, transient or partial reversal of flow), and stage III (complete steal, permanent reversal of flow).
When the collateral flow directs a large amount of flow into the subclavian artery and away from the brain, neurologic symptoms can occur. Such symptoms have been reported to occur in approximately 36% of patients.5 Often, the circle of Willis can provide enough collateral circulation to the brainstem to avert neurologic symptoms. If the posterior communicating artery is stenotic, occluded, or absent, or if there is concomitant carotid disease, then neurologic symptoms are more likely to occur.
MANIFESTATIONS OF DISEASE
Clinical Presentation
Most patients with reversal of flow in the vertebral artery have neurologic symptoms.5 In the absence of neurologic symptoms, patients are said to have subclavian steal phenomenon.
Neurologic symptoms of subclavian steal syndrome include lightheadedness, dizziness, vertigo, upper extremity numbness, visual alterations, transient ischemic attacks and, rarely, seizures or stroke.6–8 Ipsilateral upper extremity exercise increases the blood flow demand in the subclavian artery and can cause transient neurologic symptoms caused by an increase in diversion of intracranial blood flow.9
On physical examination, subclavian steal may manifest with a subclavian artery bruit or reduced blood pressure in the ipsilateral upper extremity, along with weakness of the radial pulse.10
Imaging Techniques and Findings
Ultrasound
Sonography is the initial imaging examination when subclavian steal syndrome is suspected. Ultrasound with pulsed Doppler spectral analysis can demonstrate patency and flow direction in the vertebral artery and can establish the presence of subclavian steal.11,12
Subclavian steal phenomenon is associated with specific vertebral artery waveforms. There are four types of waveforms that indicate the degree of abnormal hemodynamics11:
In occult steal (Branchereau stage I),4 the pulsed wave Doppler spectrum typically demonstrates antegrade vertebral flow with midsystolic deceleration.11,12 The waveform may show a reversed late systolic flow as a response to reactive hyperemia in the upper extremity after arm exercise (see Fig. 96-1B). In partial subclavian steal (stage II), pulsed wave Doppler depicts partial flow reversal. The Doppler waveform in occult and partial subclavian steal has been described as the bunny rabbit sign because of its resemblance to the outline of a rabbit (Fig. 96-1A).11,12
