CHAPTER 26 Stridor
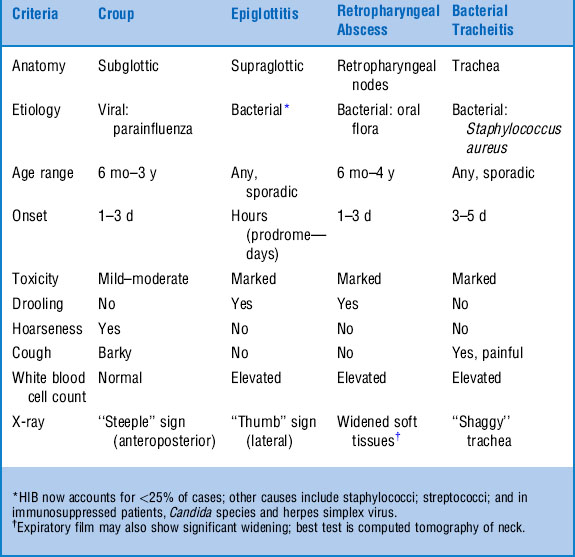
1 What are the four primary diagnostic considerations in a febrile child with acute stridor?




TABLE 26-1 illustrates clinical criteria helpful in distinguishing among the four.
2 What is the most common cause of stridor in the pediatric population?
eMedicine: Stridor. Available at www.emedicine.com/ped/topic2159.htm.
3 Name three animal sounds to which the croup cough has been compared.
The bark of a seal or sea lion, the bark of a dog, and the honking of a goose.
5 What is the characteristic radiographic finding in a patient with croup? In epiglottitis?
The classic radiographic finding in croup is the “steeple sign,” a narrowing of the laryngotracheal air column just below the vocal cords on an anterior-posterior view (Fig. 26-1). Another finding includes “ballooning” (distention) of the hypopharynx during inspiration, seen on a lateral view. The steeple sign has been show to lack sensitivity and specificity. The primary reason for obtaining radiographs in children with suspected croup should be to evaluate the possibility of other causes of stridor in atypical cases. The classic finding in epiglottitis is the “thumb sign,” referring to the lateral view of the swollen epiglottis resembling a lateral view of one’s thumb (Fig. 26-2). The thumb sign is also subjective, and radiographs alone should not be used to diagnose epiglottitis. If clinical suspicion is high, imaging should be deferred in favor of direct visualization of the airway under controlled circumstances.


6 Which bacterial infection of the upper airway most closely clinically mimics croup: Epiglottitis, bacterial tracheitis, or retropharyngeal abscess?
11 Where in the airway is the likely site of pathology in a patient with stridor that is loudest in the expiratory phase?
KEY POINTS: CLINICAL CLUES TO THE ETIOLOGY OF STRIDOR
1 Hoarseness in the presence of stridor indicates vocal cord inflammation and is reassuring for the lack of supraglottic pathology, such as epiglottitis or retropharyngeal abscess.
2 Conversely, drooling with stridor is concerning for supraglottic obstruction.
3 Inspiratory stridor suggests an extrathoracic lesion (e.g., laryngeal, nasal, pharyngeal).
4 Expiratory stridor implies an intrathoracic lesion (e.g., tracheal, bronchial).
5 Biphasic stridor may represent subglottic or glottic pathology.









