[level-membership-for-radiology-category] Most common in abdomen/pelvis (65% of cases)
Usually located within peritoneal cavity (greater omentum, bowel serosa, parietal peritoneum, undersurface of diaphragm)
Less common locations include thorax (usually after diaphragmatic rupture) and subcutaneous soft tissues
• MDCT: Multiple nodules or masses scattered throughout abdomen or pelvis (usually peritoneal cavity)
Should follow appearance of spleen on all phases of enhancement
Slightly hypoattenuating (5-10 HU less) compared to liver on NECT, striated enhancement on arterial phase, and homogeneous enhancement on venous/delayed phases
• MR: Follows appearance and enhancement of normal spleen on all sequences
• Can mimic peritoneal carcinomatosis or primary malignancies on CT and PET
• No other clinical significance in most cases
• Most patients are asymptomatic, but rarely, symptoms are due to hemorrhage, rupture, torsion, infarction, or bowel obstruction
(Left) Axial CECT demonstrates absence of the spleen (patient had a history of prior splenectomy for trauma) with small enhancing nodules in the left upper quadrant. Splenosis is not infrequently seen in close proximity to the splenectomy bed.
(Right) Axial CECT in the same patient shows additional splenic implants along the serosal surface of the left colon and along the posterior margin of the right liver lobe. Splenosis is most commonly seen within the peritoneal cavity, with extraperitoneal splenosis more rare.
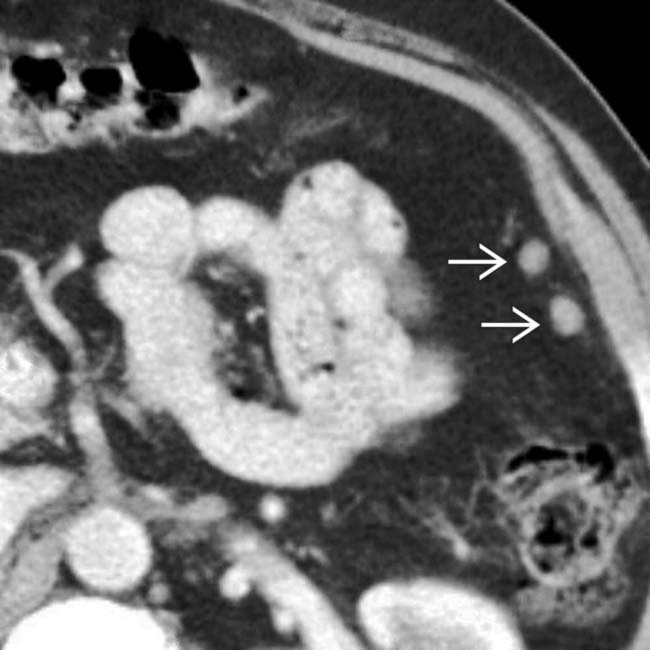
(Left) Axial CECT in a patient with remote history of abdominal trauma shows multiple soft tissue nodules along the peritoneal surfaces, which might be mistaken for carcinomatosis, but represent splenosis.
(Right) Axial CECT shows an enhancing soft tissue nodule in the left cardiophrenic angle. The patient had a distant history of traumatic splenic injury with diaphragmatic rupture, the most common reason for thoracic splenosis. Thoracic splenosis is quite rare compared to abdominal/pelvic splenosis.
TERMINOLOGY
Definitions
• Dissemination of splenic tissue into ectopic locations following splenic rupture (either traumatic or iatrogenic)
IMAGING
General Features
• Location
Most common in abdomen/pelvis (65% of cases)
– Usually located within peritoneal cavity (greater omentum, bowel serosa, parietal peritoneum, undersurface of diaphragm)
– Involvement of extraperitoneal spaces uncommon
Can occur in virtually every compartment of body
– Less common locations include thorax (usually after diaphragmatic rupture), subcutaneous soft tissues, and even intracranial cavity
• Size
Few mm to 12 cm; usually < 3 cm
• Morphology
Round or ovoid nodules; usually multiple
CT Findings
• Multiple nodules scattered throughout abdomen or pelvis
• Nodules follow appearance of spleen on all phases
Slightly hypoattenuating (5-10 HU less) compared to liver on NECT, striated enhancement on arterial phase, and homogeneous enhancement on venous/delayed phases
MR Findings
• Follows signal/enhancement of spleen on all sequences
• T1WI: Hypointense to liver; slightly hyperintense to muscle
• T2WI: Hyperintense to liver
Ultrasonographic Findings
• Nonspecific round/oval, homogeneous mass(es)
Nuclear Medicine Findings
• PET
Splenosis nodules can be FDG avid and mimic neoplasm
• Tc-99m sulfur colloid
↑ uptake within splenic nodules (similar to native spleen)
• Tc-99m labeled heat-denatured RBC scintigraphy
↑ sensitivity/specificity with ↑ uptake within nodules
90% of damaged RBCs are sequestered by splenic tissue
Imaging Recommendations
• Best imaging tool
Tc-99m labeled heat-denatured RBC scan
DIFFERENTIAL DIAGNOSIS
Peritoneal Carcinomatosis
• History of primary cancer (no history of splenic rupture)
• Usually associated with ascites, omental/peritoneal stranding and nodularity, and known history of underlying malignancy
• Tc-99m-tagged RBC scan is definitive in excluding splenosis
Accessory Spleen
• Congenital ectopic splenic tissue due to failure in fusion of splenic foci during development
• Most cases are small, solitary, and adjacent to splenic hilum
• May hypertrophy after splenectomy and mimic splenosis
• No history of trauma
Polysplenia
• Multiple small spleens associated with abdominal situs inversus and cardiovascular anomalies
Visceral Mass or Malignancy
• Splenosis can mimic pancreatic, adrenal, renal, and gastric masses (and vice versa)
Splenosis abutting pancreatic tail can mimic neuroendocrine tumor
• CT/MR enhancement characteristics and nuclear scintigraphy helpful in differentiation
Peritoneal Endometriosis
• Soft tissue nodules with variable enhancement usually located in pelvis (uterine ligaments, cul-de-sac, fallopian tubes, etc.)
• No history of trauma
PATHOLOGY
General Features
• Etiology
Blunt traumatic disruption of splenic capsule with seeding of tissue into peritoneal cavity
– Hematogenous spread may also play a role
Does not occur after elective splenectomy (no rupture of capsule)
Gross Pathologic & Surgical Features
• Reddish-blue color; no capsule
• Supplied by small perforating vessels from local tissues
Not supplied by splenic artery branches, unlike splenule
Microscopic Features
• May completely resemble normal splenic tissue
Cannot differentiate from splenule based on histology
• Distorted architecture with no hilum
• No capsule or poorly formed capsule
• Poorly formed white pulp
• ↓ elastic content
CLINICAL ISSUES
Presentation
• Most common signs/symptoms
• Most are asymptomatic
• Rarely symptomatic due to hemorrhage, rupture, torsion, infarction, or bowel obstruction
Demographics
• Epidemiology
Most cases reported in adults; M > F (↑ trauma in men)
∼ 70% of patients with splenectomy following trauma
70% of reported cases suffered trauma during teenage years
Usually detected years after trauma
– Mean time after trauma: 10 years; range: 5 months-32 years
Natural History & Prognosis
• No clinical significance in most cases
• Recurrent disease after splenectomy with hematologic disorders (idiopathic thrombocytic purpura, lymphoma, etc.)
• No Howell-Jolly bodies, Heinz bodies, or abnormal RBCs on peripheral blood smear despite splenectomy
Indicates patient has functioning spleen
Treatment
• In most cases, no treatment is necessary
• Surgical resection only if complications or symptoms are present
Axial CECT in a patient with splenosis shows implants in the left upper quadrant . In an oncology patient, these could easily be mistaken for peritoneal implants of cancer.
Axial CECT in a 37-year-old woman shows multiple spherical, soft tissue density masses throughout the peritoneal cavity. The spleen is absent, with a remote history of blunt abdominal trauma.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Most common in abdomen/pelvis (65% of cases)
Usually located within peritoneal cavity (greater omentum, bowel serosa, parietal peritoneum, undersurface of diaphragm)
Less common locations include thorax (usually after diaphragmatic rupture) and subcutaneous soft tissues
• MDCT: Multiple nodules or masses scattered throughout abdomen or pelvis (usually peritoneal cavity)
Should follow appearance of spleen on all phases of enhancement
Slightly hypoattenuating (5-10 HU less) compared to liver on NECT, striated enhancement on arterial phase, and homogeneous enhancement on venous/delayed phases
• MR: Follows appearance and enhancement of normal spleen on all sequences
• Can mimic peritoneal carcinomatosis or primary malignancies on CT and PET
• No other clinical significance in most cases
• Most patients are asymptomatic, but rarely, symptoms are due to hemorrhage, rupture, torsion, infarction, or bowel obstruction
(Left) Axial CECT demonstrates absence of the spleen (patient had a history of prior splenectomy for trauma) with small enhancing nodules in the left upper quadrant. Splenosis is not infrequently seen in close proximity to the splenectomy bed.
(Right) Axial CECT in the same patient shows additional splenic implants along the serosal surface of the left colon and along the posterior margin of the right liver lobe. Splenosis is most commonly seen within the peritoneal cavity, with extraperitoneal splenosis more rare.
(Left) Axial CECT in a patient with remote history of abdominal trauma shows multiple soft tissue nodules along the peritoneal surfaces, which might be mistaken for carcinomatosis, but represent splenosis.
(Right) Axial CECT shows an enhancing soft tissue nodule in the left cardiophrenic angle. The patient had a distant history of traumatic splenic injury with diaphragmatic rupture, the most common reason for thoracic splenosis. Thoracic splenosis is quite rare compared to abdominal/pelvic splenosis.
TERMINOLOGY
Definitions
• Dissemination of splenic tissue into ectopic locations following splenic rupture (either traumatic or iatrogenic)
IMAGING
General Features
• Location
Most common in abdomen/pelvis (65% of cases)
– Usually located within peritoneal cavity (greater omentum, bowel serosa, parietal peritoneum, undersurface of diaphragm)
– Involvement of extraperitoneal spaces uncommon
Can occur in virtually every compartment of body
– Less common locations include thorax (usually after diaphragmatic rupture), subcutaneous soft tissues, and even intracranial cavity
• Size
Few mm to 12 cm; usually < 3 cm
• Morphology
Buy Membership for Radiology Category to continue reading. Learn more here
 Usually located within peritoneal cavity (greater omentum, bowel serosa, parietal peritoneum, undersurface of diaphragm)
Usually located within peritoneal cavity (greater omentum, bowel serosa, parietal peritoneum, undersurface of diaphragm) Less common locations include thorax (usually after diaphragmatic rupture) and subcutaneous soft tissues
Less common locations include thorax (usually after diaphragmatic rupture) and subcutaneous soft tissues



 in the left upper quadrant. Splenosis is not infrequently seen in close proximity to the splenectomy bed.
in the left upper quadrant. Splenosis is not infrequently seen in close proximity to the splenectomy bed.
 along the serosal surface of the left colon and along the posterior margin of the right liver lobe. Splenosis is most commonly seen within the peritoneal cavity, with extraperitoneal splenosis more rare.
along the serosal surface of the left colon and along the posterior margin of the right liver lobe. Splenosis is most commonly seen within the peritoneal cavity, with extraperitoneal splenosis more rare.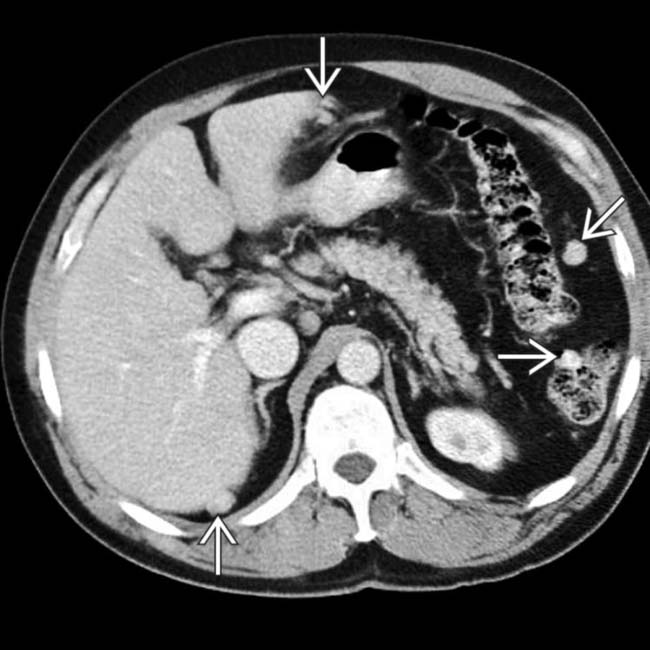
 along the peritoneal surfaces, which might be mistaken for carcinomatosis, but represent splenosis.
along the peritoneal surfaces, which might be mistaken for carcinomatosis, but represent splenosis.
 in the left cardiophrenic angle. The patient had a distant history of traumatic splenic injury with diaphragmatic rupture, the most common reason for thoracic splenosis. Thoracic splenosis is quite rare compared to abdominal/pelvic splenosis.
in the left cardiophrenic angle. The patient had a distant history of traumatic splenic injury with diaphragmatic rupture, the most common reason for thoracic splenosis. Thoracic splenosis is quite rare compared to abdominal/pelvic splenosis.




















 . In an oncology patient, these could easily be mistaken for peritoneal implants of cancer.
. In an oncology patient, these could easily be mistaken for peritoneal implants of cancer.
 throughout the peritoneal cavity. The spleen is absent, with a remote history of blunt abdominal trauma.
throughout the peritoneal cavity. The spleen is absent, with a remote history of blunt abdominal trauma.