Low-attenuation complex fluid collection ± air-fluid levels


 May extend to subcapsular location and may rarely cause splenic rupture with generalized peritonitis
May extend to subcapsular location and may rarely cause splenic rupture with generalized peritonitis

• Echinococcal (hydatid) cyst on CECT



PATHOLOGY
• Multiple different causes for splenic pyogenic abscesses



 within the spleen that proved to be a pyogenic abscess. Such large abscesses are unusual in the spleen, especially in the absence of prior splenic infarction.
within the spleen that proved to be a pyogenic abscess. Such large abscesses are unusual in the spleen, especially in the absence of prior splenic infarction.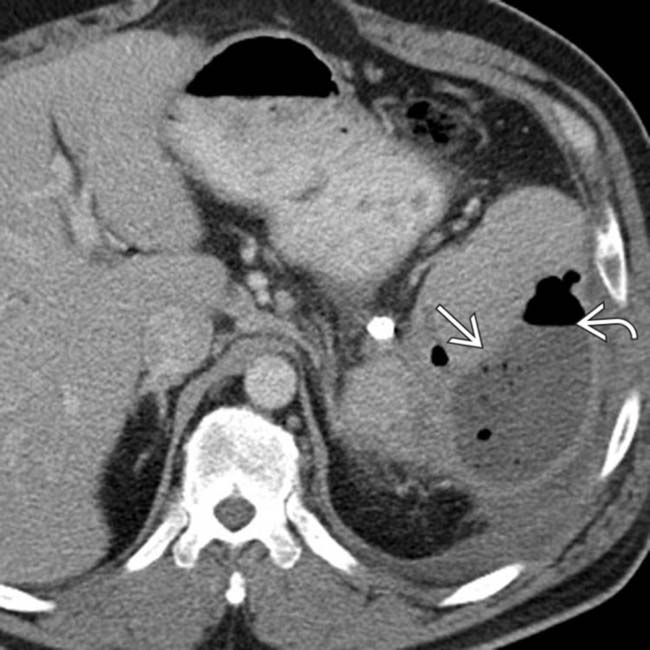
 demonstrates a rim-enhancing fluid collection with an air-fluid level
demonstrates a rim-enhancing fluid collection with an air-fluid level  , consistent with a splenic abscess. The patient was treated with percutaneous drainage and antibiotics.
, consistent with a splenic abscess. The patient was treated with percutaneous drainage and antibiotics.
 throughout the spleen. The patient deteriorated rapidly, and multiple tuberculous abscesses were identified at autopsy.
throughout the spleen. The patient deteriorated rapidly, and multiple tuberculous abscesses were identified at autopsy.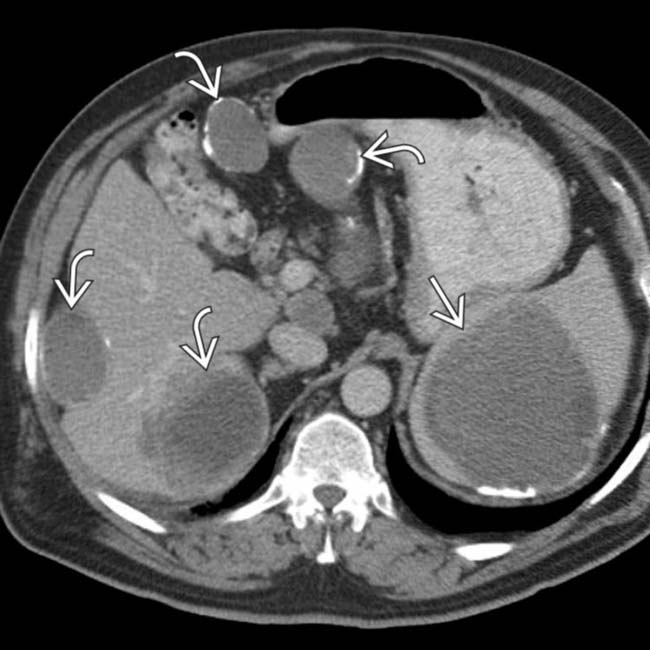
 with additional similar lesions in the liver and peritoneal cavity
with additional similar lesions in the liver and peritoneal cavity  , many of which have calcified walls. This patient had a prior rupture of a hepatic hydatid cyst with diffuse spread throughout the abdomen.
, many of which have calcified walls. This patient had a prior rupture of a hepatic hydatid cyst with diffuse spread throughout the abdomen.IMAGING
General Features






CT Findings
• Pyogenic abscess





• Echinococcal (hydatid) cyst
 Complex cyst with multiple low density “daughter” cysts and thick, enhancing wall composed of fibrous tissue (“cyst within a cyst” appearance)
Complex cyst with multiple low density “daughter” cysts and thick, enhancing wall composed of fibrous tissue (“cyst within a cyst” appearance)
 Serpiginous, linear hypodense bands within cyst due to collapsed parasitic membranes (water lily sign)
Serpiginous, linear hypodense bands within cyst due to collapsed parasitic membranes (water lily sign)
Complex cyst with multiple low density “daughter” cysts and thick, enhancing wall composed of fibrous tissue (“cyst within a cyst” appearance) Serpiginous, linear hypodense bands within cyst due to collapsed parasitic membranes (water lily sign)










DIFFERENTIAL DIAGNOSIS
Splenic Infarct





PATHOLOGY
General Features



























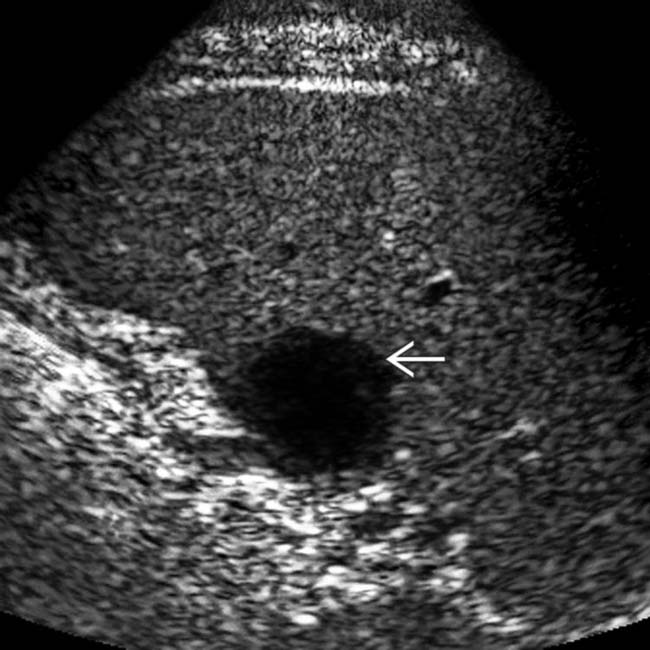
 and a thick irregular wall
and a thick irregular wall  . The adjacent splenic parenchyma
. The adjacent splenic parenchyma  appears normal. Note the typical avascular nature of the abscess.
appears normal. Note the typical avascular nature of the abscess.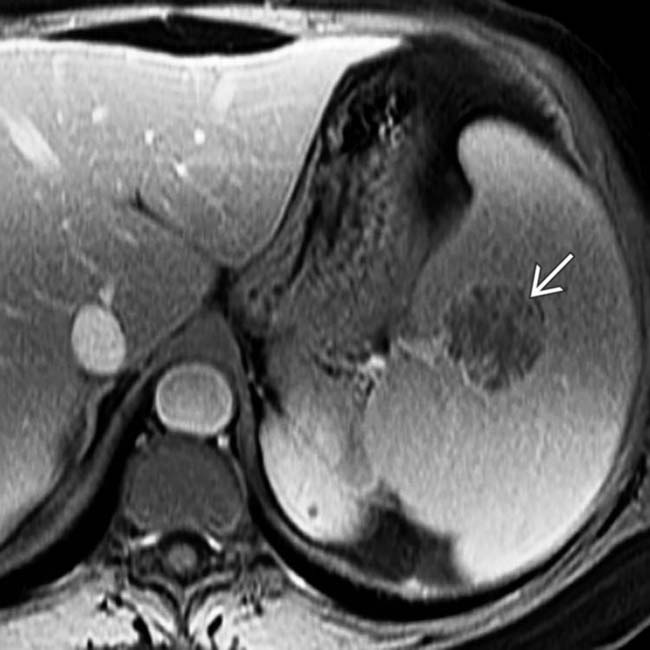
 . Blood cultures identified Staphylococcus and the patient recovered with antibiotics.
. Blood cultures identified Staphylococcus and the patient recovered with antibiotics.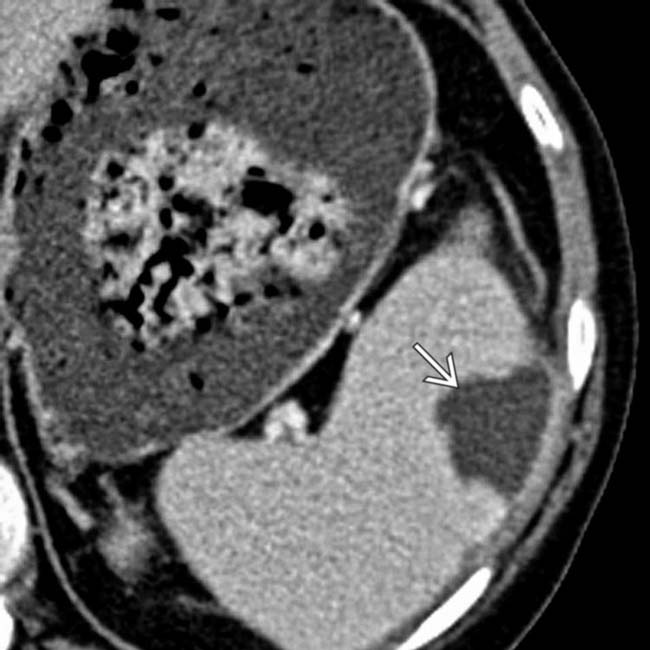
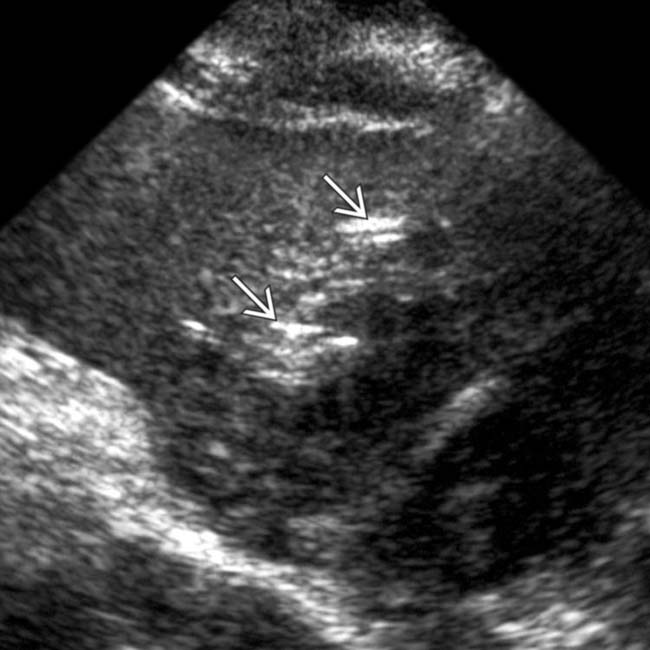
 in the periphery of the spleen’s midportion; findings that are consistent with an abscess.
in the periphery of the spleen’s midportion; findings that are consistent with an abscess.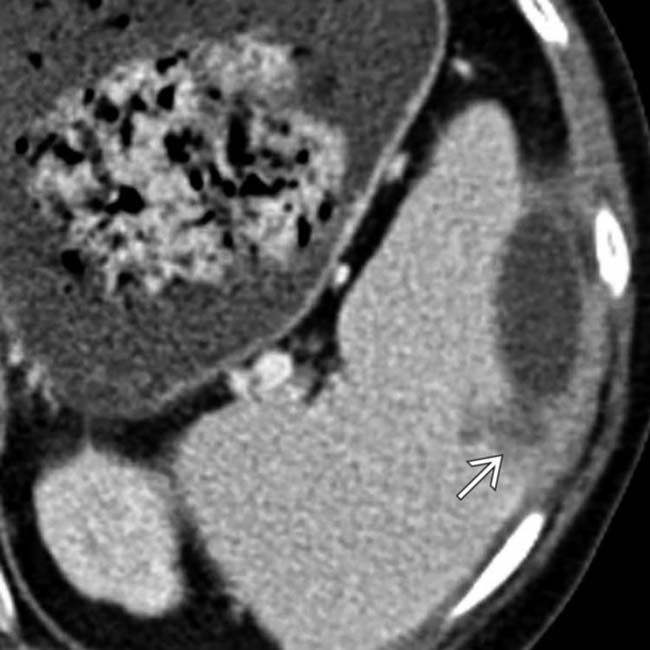
 , suggesting a possible abscess rupture. An echocardiogram showed multiple vegetations in both the aortic and mitral valves, suggesting that this abscess is due to underlying endocarditis.
, suggesting a possible abscess rupture. An echocardiogram showed multiple vegetations in both the aortic and mitral valves, suggesting that this abscess is due to underlying endocarditis.
 .
.
 as well. The patient underwent an echocardiogram, which additionally revealed aortic valve vegetations from endocarditis (not shown).
as well. The patient underwent an echocardiogram, which additionally revealed aortic valve vegetations from endocarditis (not shown).
 and fewer, similar lesions in the liver
and fewer, similar lesions in the liver  .
.
 . Liver biopsy and blood cultures confirmed a systemic infection with histoplasmosis.
. Liver biopsy and blood cultures confirmed a systemic infection with histoplasmosis.
 .
.
 .
.
 .
.

 .
.
 .
.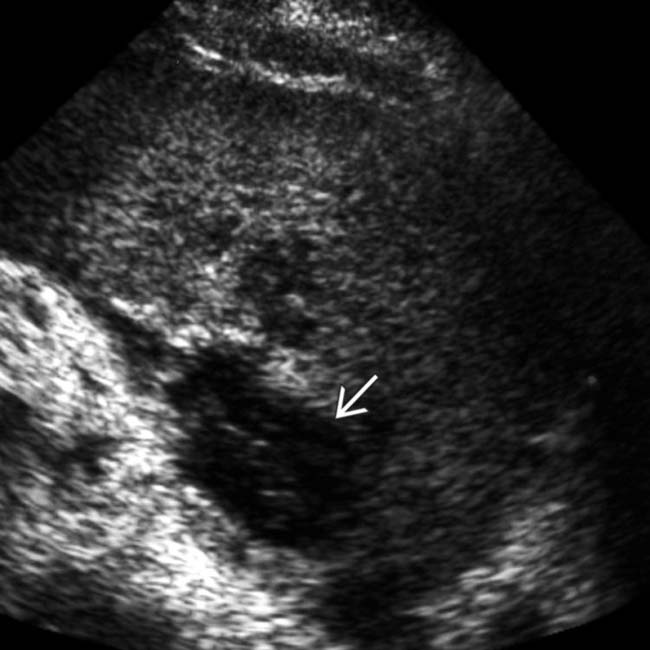
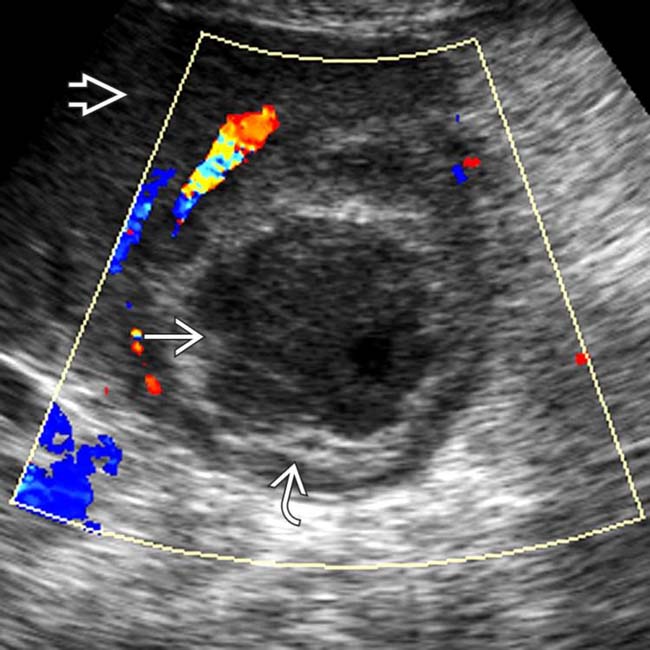
 with little distal acoustic enhancement.
with little distal acoustic enhancement.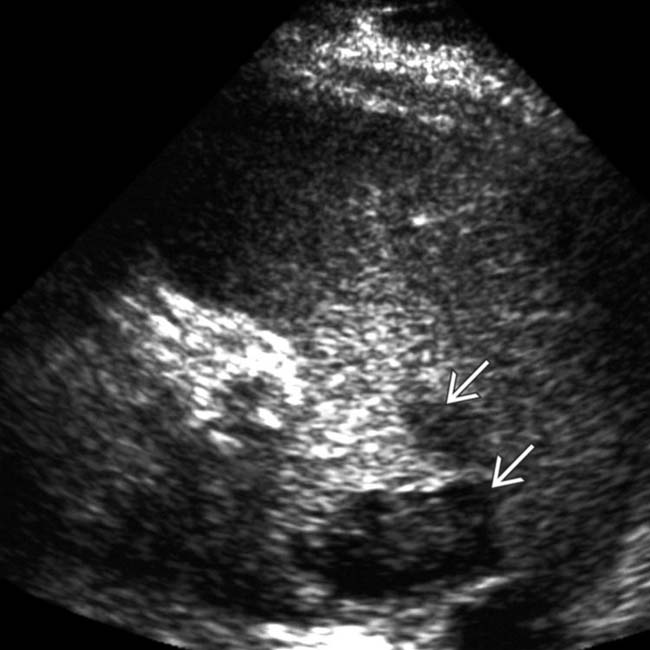
 .
.
 in the midportion of the spleen, findings consistent with an abscess.
in the midportion of the spleen, findings consistent with an abscess.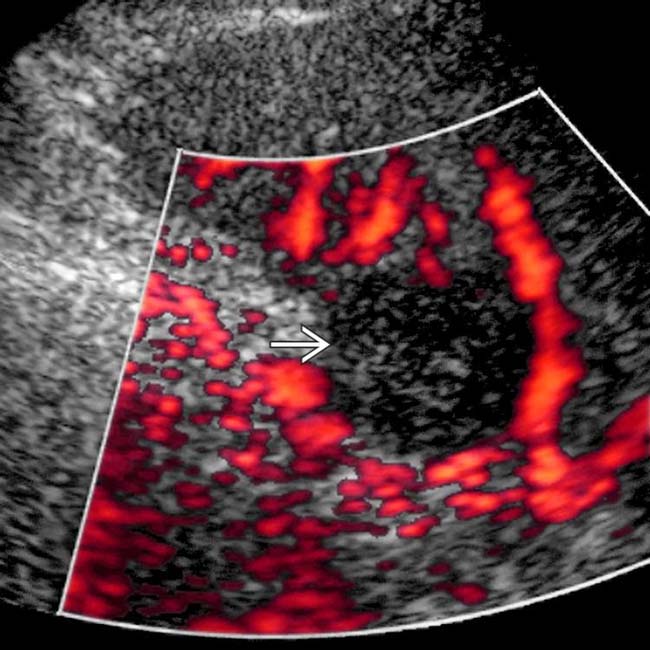
 , which excludes a solid lesion such as lymphoma or metastasis. Blood cultures were positive for anaerobic Streptococcus, and the lesion resolved with antibiotic therapy.
, which excludes a solid lesion such as lymphoma or metastasis. Blood cultures were positive for anaerobic Streptococcus, and the lesion resolved with antibiotic therapy.

