Speech and higher function
Speech and higher function are not formally examined in every neurological patient. This should be undertaken in patients who report difficulties or if an abnormality is suggested by the history. Abnormalities in these areas can explain difficulties in obtaining a clear history. If in doubt, test.
Speech
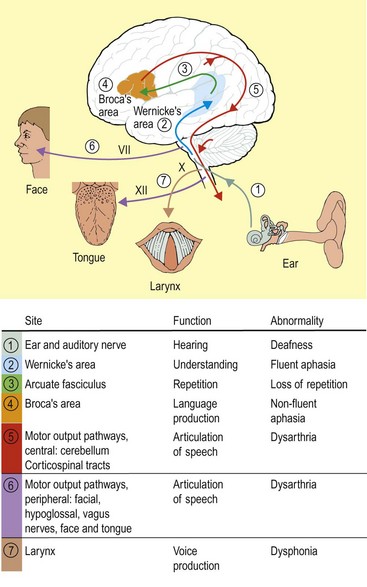
Speech is required for the patient to give a history and it therefore constitutes the first part of the examination. The processes in language and terms used to describe abnormalities are summarized in Figure 1. Speech processing occurs in the dominant hemisphere. The process of understanding occurs in Wernicke’s area in the supramarginal gyrus of the parietal lobe and the upper temporal lobe. This is linked by the arcuate fasciculus to Broca’s area in the inferior frontal gyrus where speech output is generated. This then requires motor output involving corticospinal tracts, the basal ganglia and cerebellar inputs. The larynx is innervated by the vagus nerve to produce the voice, and then the tongue and lips, innervated by the hypoglossal and facial nerves, produce articulated speech (Fig. 1).
Higher function



Factors affecting assessment of higher function
Memory
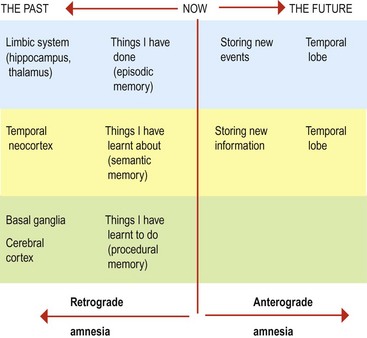
Memory is complicated and can be classified in several ways (Fig. 2). The content of the memory can be divided into: