15 Small Intestine Diseases
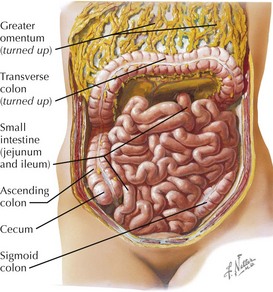
Anatomy of the Small Intestine
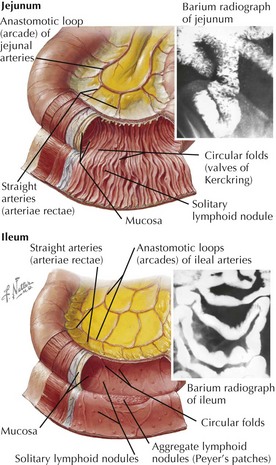
Jejunum
Ileum
Microscopic Anatomy





• Submucosa: strongest layer, connective tissue, Meissner’s plexus (parasympathetic ganglion cells and neuronal network)



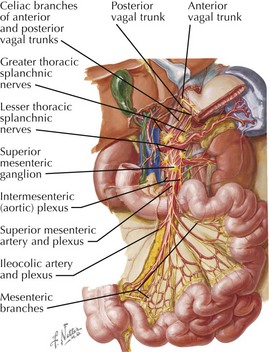
Innervation
• Parasympathetic: vagus


• Sympathetic




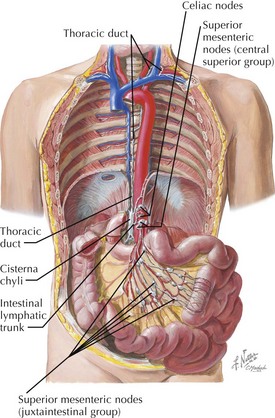
Vessels and Lymphatics
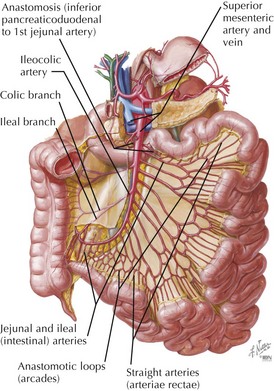
Arterial Supply



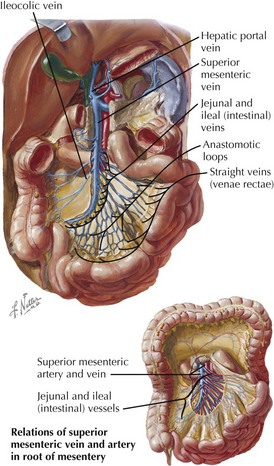
Venous Drainage
• Duodenal veins empty into splenic vein, superior mesenteric vein, and portal vein (which lies posterior to the first part).
Clinical Correlates
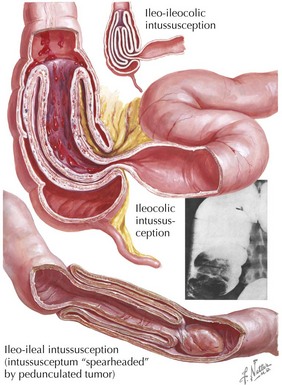
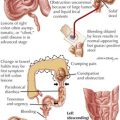
Intussusception
• Portion of bowel (intussusceptum) invaginates into an adjoining segment of bowel (intussuscipiens), causing obstruction.










Diverticular Disease


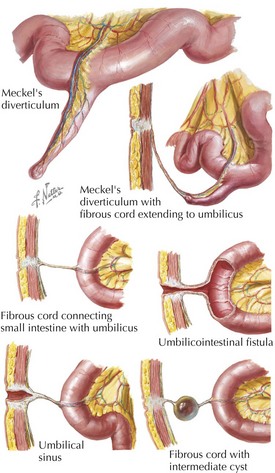
Meckel’s Ileal Diverticulum
• Can also include gastric tissue: symptomatic with ulcer occurring in opposite gut wall (due to acid secretion)
Cancer of the Small Intestine
• Most common malignant neoplasms: adenocarcinomas, carcinoid tumors, lymphomas, and gastrointestinal stroma tumors, all rare
• Carcinoid





• Gastrointestinal stromal tumors (GIST): most common GI mesenchymal neoplasm (1% of all), often associated with Kit gene mutation





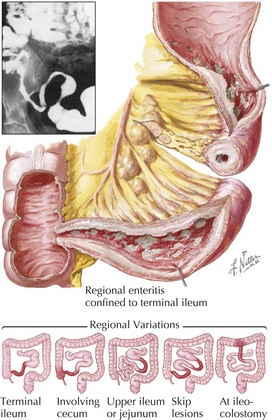
Crohn’s Disease
Short-Bowel Syndrome
• Because of absorptive and vascular reserve capacity of small intestine, limited resection of bowel is generally associated with minimal morbidity.
• Extensive resection can result in short-bowel syndrome, with insufficient absorptive activity, intractable diarrhea, malnutrition, weight loss, and dehydration.