Small Bowel Repair/Resection
Brian J. Albers  David J. Lamon
David J. Lamon
The small intestine is a continuation of the gastrointestinal (GI) tract, extending from the duodenal bulb to the ileocecal valve. It comprises the luminal mucosa, an inner circular layer and outer longitudinal layer of muscle, and the external serosa. For surgical purposes, the small bowel has two layers: the inner mucosa and the outer serosa. Blood is supplied by the mesentery, whose vessel of origin is the superior mesenteric artery and vein.
Isolation of the segment to be resected is done with noncrushing clamps across the bowel proximally and distally (Fig. 94–1). The mesentery is taken down with clamps and ligated with 2–0 silk free ties (Figs. 94–2 and 94–3). If a handsewn anastomosis is desired, the bowel is sharply divided along the edge of a noncrushing clamp. The injured segment is removed, and the two ends of remaining small bowel are opposed and held aligned with traction sutures of 3-0 silk (Fig. 94–4). Circumferential, single-layer, 3-0 silk, interrupted sutures are used for the anastomosis (Fig. 94–5) with inversion of the mucosa (Fig. 94–6). All sutures are placed under direct visualization (Fig. 94–7), with palpable confirmation of a patent anastomotic ring (Fig. 94–8). The mesenteric defect is then closed to prevent internal herniation (Fig. 94–9).
If a stapled anastomosis is planned, the resected segment is excised with successive firing of a GIA 75-mm stapling device. The proximal and distal segments are then affixed in parallel with seromuscular sutures at the inner mesenteric border (Figs. 94–10 and 94–11). Enterotomies are created to admit the stapler (Fig. 94–12), which is fired as the bowel segments are rotated to oppose the antimesenteric borders of each segment (Fig. 94–13). The anastomosis is briefly inspected for significant mucosal bleeding. If none is found, the enterotomy is then grasped with Allis clamps. The edges are opposed perpendicular to the direction of the side-to-side anastomosis just created (Fig. 94–14). Firing the GIA across and under the clamps creates a functional end-to-end anastomosis (Fig. 94–15). The mesenteric rent is then closed.
Repair of a transmural injury may be performed on unprepped small bowel with minimal risk, as long as good technique is used. The edges of the perforated bowel should be trimmed before suturing. Simple transmural lacerations not involving the mesentery may be closed transversely (Heineke-Mikulicz operation closing the wound so as not to constrict the lumen) by placement of corner traction sutures and single-layer interrupted 3-0 silk (Figs. 94–16 and 94–17). Multiple focal injuries or devascularization requires resection with anastomosis. This can be handsewn or stapled, with similar results.

FIGURE 94–1 The segment to be resected is isolated from enteric flow by application of proximal and distal noncrushing clamps to prevent further contamination.
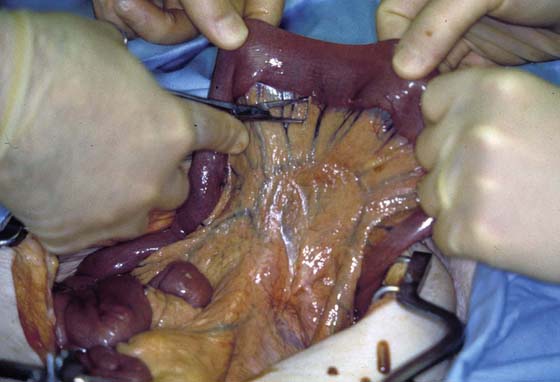
FIGURE 94–2 A defect in the mesenteric border is created at the proximal and distal ends to be resected, staying close to the bowel wall.
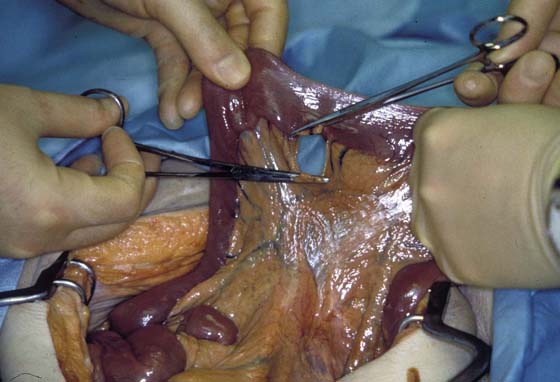
FIGURE 94–3 The mesentery is then taken down between clamps and ligated with 2-0 silk suture.
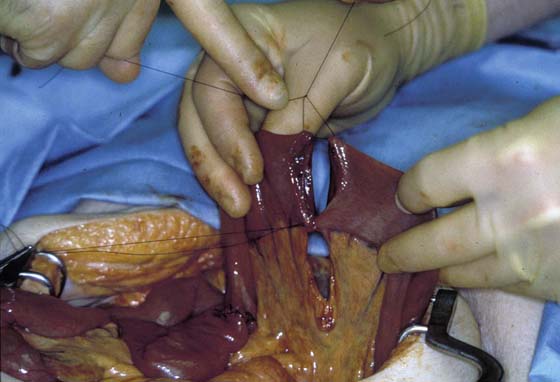
FIGURE 94–4 Once devascularized, the bowel segment is excised sharply. Mucosal bleeding should be evident from the opposed ends to be anastomosed. Brisk mucosal bleeding can be controlled with judicious use of electrocautery. The ends of the bowel to be anastomosed are aligned and held in place with 3-0 silk traction sutures placed at the mesenteric and antimesenteric borders.

FIGURE 94–5 Single-layer, interrupted 3-0 silk sutures are used to perform the anastomosis. Care is taken to incorporate 4 to 5 mm of serosa and just the edge of the mucosa with each needle throw through the bowel edges. Knots are tied on the outside and are spaced 4 mm apart.

FIGURE 94–6 When the anastomotic suture is tied, care is taken to invert the mucosa while setting the knot.
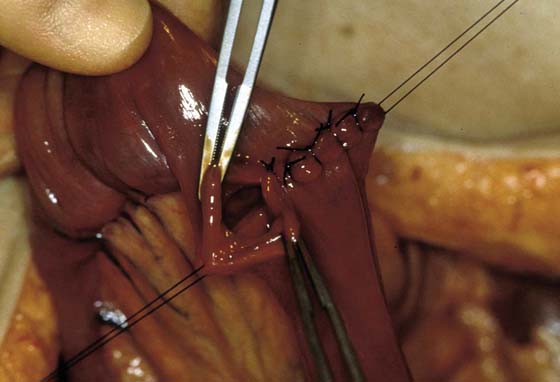
FIGURE 94–7 Nearing completion of the anastomosis, the last several sutures are left untied until the last suture is placed to permit full visualization of each needle throw. Inspect the corner suture placement carefully to ensure there are no gaps.

FIGURE 94–8 Once completed, the anastomosis is inspected circumferentially. Any gaps between sutures are filled with 3-0 silk interrupted serosal sutures placed superficially, taking care not to encroach on the lumen. The anastomotic ring is palpated, and continuity is ensured by admittance of a fingertip through the ring. The traction sutures are then tied and cut.
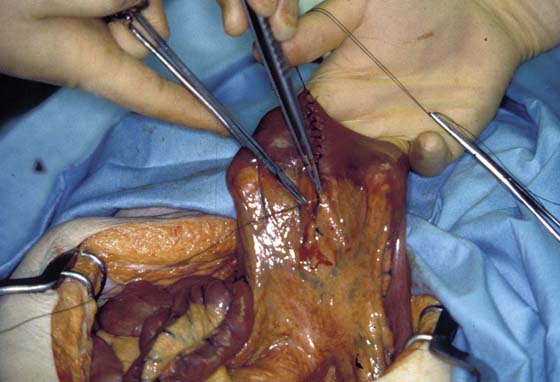
FIGURE 94–9 The mesenteric defect is then closed with interrupted 3-0 silk sutures, incorporating only the peritoneum and avoiding the underlying vessels.
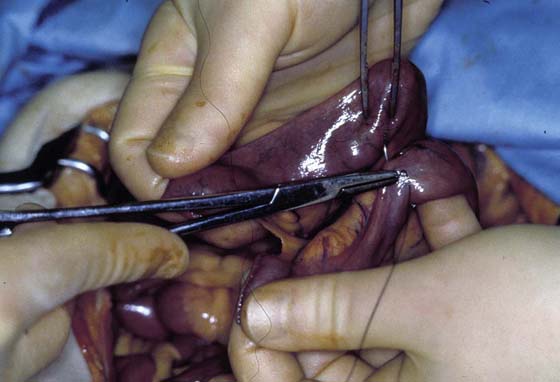
FIGURE 94–10 The proximal and distal portions of divided small bowel are held parallel to each other. A single seromuscular 3-0 silk traction suture is placed at the inner mesenteric border, joining the two segments approximately 100 mm from the stapled edge.
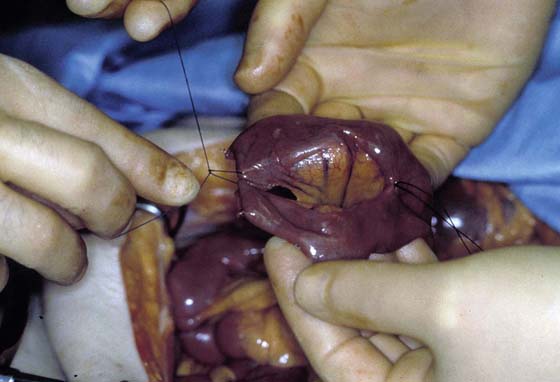
FIGURE 94–11 Another seromuscular traction suture is placed at the inner mesenteric border, near the mesenteric side of the staple lines.

FIGURE 94–12 The antimesenteric edge of each staple line is then sharply opened only enough to permit entry of the GIA stapling device (75 mm).

FIGURE 94–13 The stapling anvil and cartridge are placed into each limb of the bowel as shown. Downward traction is then applied to the previously placed mesenteric traction sutures, thereby rotating the bowel so that the antimesenteric bowel borders are opposed between the jaws of the stapler. Once the operator is satisfied that no mesenteric fat is caught in the staple line, as evidenced by the ability to run a finger along both sides of the stapler while touching only serosa, the stapling device is fired.
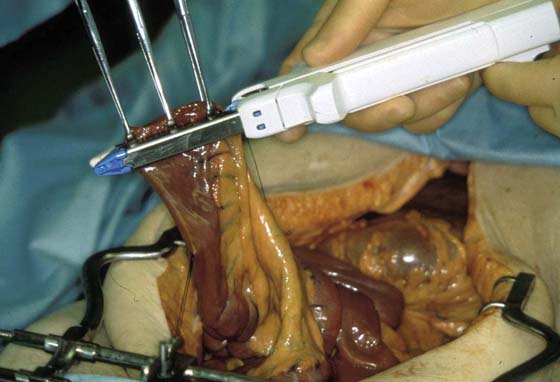
FIGURE 94–14 Once the fired stapler is removed, the side-to-side small bowel anastomosis can be visually inspected for significant mucosal bleeding. If none is found, several Allis clamps are used to grasp the enterotomy edges in a fashion that incorporates generous amounts of serosa perpendicular to the direction of the side-by-side anastomosis. Ideally this should incorporate the staple lines from the original resection edges, as well as the traction sutures adjacent to these.

FIGURE 94–15 The stapler is reloaded, positioned as described, and is fired, with the resulting side-to-side, now functional end-to-end anastomosis appearing like this. Inspect the stapled edges carefully, milking enteric contents through the anastomosis to check for leaks. Close the mesenteric defect as previously described.

FIGURE 94–16 A transmural laceration in the small bowel is shown. The mesentery is not involved. Simple closure is sufficient.
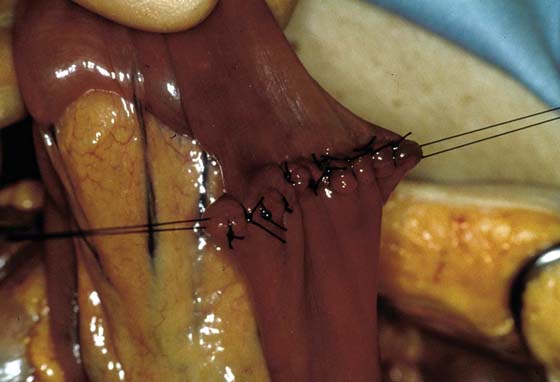
FIGURE 94–17 Corner sutures of 3-0 silk are placed and are used to elongate the laceration in a transverse fashion to facilitate closure with interrupted 3-0 silk sutures placed approximately 4 mm apart, with bites encompassing 4 to 5 mm of serosa and just the edge of the mucosa on each side of the defect. The knots are tied as the mucosa is invaginated. The repair is then checked for leaks and luminal patency.






