CHAPTER 13 Sleeve Lobectomy
Right Upper Lobe – Video 13
Approach to Video-Assisted Sleeve Lobectomy of the Right Upper Lobe
Key Points
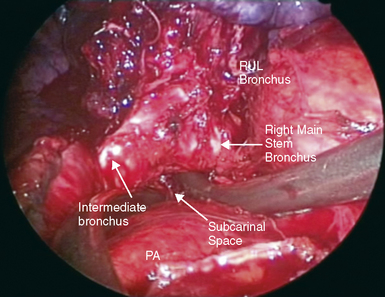
♦ The right upper lobe bronchus is posterior to the right pulmonary artery and must be separated from the artery for transection.
♦ Mediastinoscopy with a complete subcarinal node dissection mobilizes the mainstem and intermediate bronchi from the lymph nodes and pericardium. Perform the mediastinoscopy during the same anesthesia as the sleeve lobectomy because a delay between the two procedures produces adhesions that make the dissection more difficult.
 Video-Assisted Sleeve Lobectomy of the Right Upper Lobe (Video 13)
Video-Assisted Sleeve Lobectomy of the Right Upper Lobe (Video 13)
Step 2. Transection of Bronchi
♦ With a knife on a long handle through the utility incision, cut the mainstem and intermediate bronchi. Usually cut the bronchi from anterior to posterior so the cut is made away from the pulmonary artery (Figure 13-2).
Step 3. Posterior Bronchial Anastomosis
♦ Place a stay suture posteriorly on the intermediate bronchus to help approximate the intermediate and mainstem bronchi (Figure 13-3).
♦ It is not necessary to take down the inferior pulmonary ligament for a routine RUL, but it does help take tension off the anastomosis for a sleeve resection.
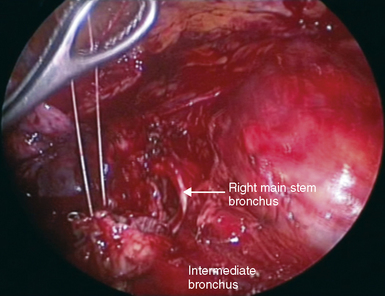
♦ Place the interrupted sutures from posterior to anterior along the membranous portion on the bronchus with a standard needle holder through the utility incision (Figure 13-4).1
4 Completion of Bronchi Anastomosis
♦ Place the sutures for the remainder of the anastomosis so the knots are tied outside the lumen (Figure 13-5).
♦ The anastomosis is close enough to a properly placed utility incision so the knots may be tied extracorporeally and then pushed with a finger through the utility incision to the anastomosis. Rarely, a knot pusher is needed.
♦ Fill the chest with water (not saline) because the red blood cells explode in water, allowing better visualization through the water to examine the anastomosis for possible bleeding or air leak.