Chapter 9 Shoulder and Elbow Reduction
Clavicle fracture
Pearls
1. Clavicle fractures with more than 1.5 cm of overlap result in long-term disability and should be treated with an open reduction and internal fixation.
2. Fractures that tent the skin can erode through the skin and are unlikely to heal without open reduction and internal fixation.
Acromioclavicular separation


Glenohumeral dislocation
Overview
Precautions
1. Confirm that no fracture is present on diagnostic films before attempting a reduction. Standard reduction maneuvers can result in a displaced four-part fracture that requires surgical fixation/prosthetic replacement.
2. Confirm that the humeral head is not impacted onto the glenoid (known as a Hill-Sachs lesion) before attempting a reduction (see Figure 9-4). Standard reduction maneuvers can result in a head-splitting fracture.
3. When applying traction, make sure that the force is applied over a broad area; otherwise, a forearm fracture can result.
4. Be aware that some persons may voluntarily initiate a glenohumeral dislocation in an effort to gain access to drugs.
5. Reducing dislocations in persons who present more than a few days after the injury may not be possible, and attempting to do so could result in a fracture; it is preferable not to attempt a reduction and to take the patient to the operating room if simple traction does not succeed in reducing the dislocation.
Pearls
1. Be patient; the stability of the shoulder is provided largely by a set of small but powerful muscles that must be overcome with gentle sustained traction before a reduction is possible.
3. For posterior dislocations, stretching the rotator cuff muscles by maximal internal rotation of the shoulder may be necessary.
Anterior glenohumeral dislocation
Detailed Technique
3. Prepare traction setup:
4. Apply traction:
a. Position yourself along the ipsilateral side of the stretcher so that the shoulder is slightly abducted.
8. Place the arm in a sling (see Chapter 13) in internal rotation or in a gunslinger brace in external rotation.






Posterior glenohumeral dislocation
Detailed Technique
3. Prepare traction setup:
4. Apply traction:
a. Position yourself along the ipsilateral side of the stretcher so that the shoulder is slightly abducted.
9. Place the arm in a sling (see Chapter 13) in internal rotation or in a gunslinger brace in external rotation.

Proximal humerus fractures
Overview
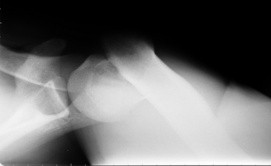
2. Closed reductions of the tuberosities cannot be maintained and should not be attempted (Figure 9-12).
3. Reducing a fracture/dislocation in a closed manner requires a high level of expertise and should only be attempted with caution.

Pearls
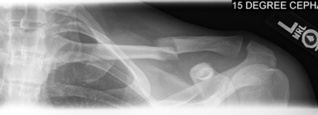
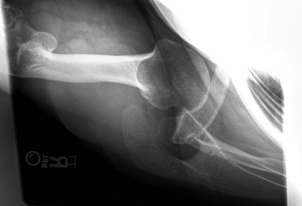
1. Always obtain an axillary view radiograph to rule out a fracture dislocation and to better visualize the humeral head (Figure 9-13).
Humeral shaft fractures
Precautions
1. The radial nerve is at risk in this type of fracture and during application of the coaptation splint.


Pearls
3. Often it is best to perform the reduction after a coaptation splint is applied but before it sets.
4. Cooperative patients can assist in the reduction by relaxing their shoulder and passively holding their elbow in a flexed position by supporting the injured hand with the uninjured hand.
5. Fractures in the distal third of the diaphysis require immobilization of the elbow in a posterior splint in addition to a coaptation splint.







Detailed Technique
2. Perform a reduction maneuver based on radiographic evidence of displacement. Most fractures require a two-point mold with one hand anterolateral at the fracture site and the other posteromedial at the elbow (Figure 9-23).
3. Bring the excess stockinette material behind the neck and down to and around the wrist and tie it back to itself to create a sling.
4. Create an abduction bump by covering a pyramid of three 4-inch-wide rolls of cast padding in more cast padding.
5. Place the abduction bump between the elbow and the body and secure it to the elbow with elastic or a self-adhesive bandage (see Figure 9-20).

Periarticular elbow fractures

Pearls
2. Because distal humeral fractures tend to displace in apex volar angulation, the elbow should be splinted in greater than 90 degrees of flexion.
3. Because proximal ulnar fractures tend to displace in apex dorsal angulation, the elbow should be splinted in less than 90 degrees of flexion in an attempt to reapproximate the fracture fragments.
4. Because radial head/neck fractures tend to displace posteriorly, a reduction maneuver should be attempted before application of a splint.

Elbow dislocations
Overview
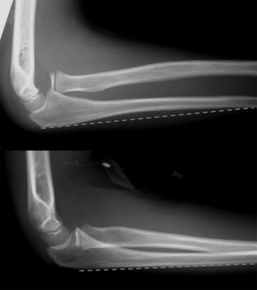
1. Elbow dislocations can occur in any direction, but most commonly the ulna dislocates posteriorly (Figure 9-26).
2. The AIN, radial nerve, and ulnar nerve are closely associated with the elbow and are at risk from the injury and the reduction.

Pearls
1. Reduction techniques should be tailored to the direction of the dislocation, with consideration of associated fractures.
2. Terrible triad injuries, which include elbow dislocation, radial head fracture, and coronoid fracture, are extremely unstable injuries, and reduction may not be able to be maintained even in elbow flexion.
3. Terrible triad injuries should be splinted in forearm pronation to tighten the lateral-sided structures.
4. Dislocations with medial epicondyle fractures, which are seen more commonly in children, are associated with ulnar nerve entrapment in the joint. Ulnar nerve dysfunction in this setting is an emergency requiring advanced imaging or exploration.
Detailed Technique
1. Position the patient standing or sitting upright if a hematoma block is to be used for anesthesia (in a cooperative patient).
2. Position the patient supine on a stretcher with the ipsilateral shoulder off the stretcher if conscious sedation is to be used.
5. If any medial/lateral translation is present, stabilize the distal humerus with one hand while grasping the proximal forearm with the other hand (Figure 9-27).
7. Feel the epicondyles and the olecranon to ensure that the olecranon is between the two epicondyles.
8. Place one hand anterior on the distal humerus and the other hand grasping the wrist (Figure 9-28).




Radial head dislocation
Precautions
Pearls
2. Beware of the plastically deformed ulna:
Detailed Technique
1. Position the patient standing or sitting upright if a hematoma block is to be used for anesthesia (in a cooperative patient).
2. Position the patient supine on a stretcher with the ipsilateral shoulder off the stretcher if conscious sedation is to be used.
7. Posterior dislocation: