[level-membership-for-orthopaedics-category]
CHAPTER FOUR SHOULDER
AXIOMS IN ASSESSING THE SHOULDER
INTRODUCTION
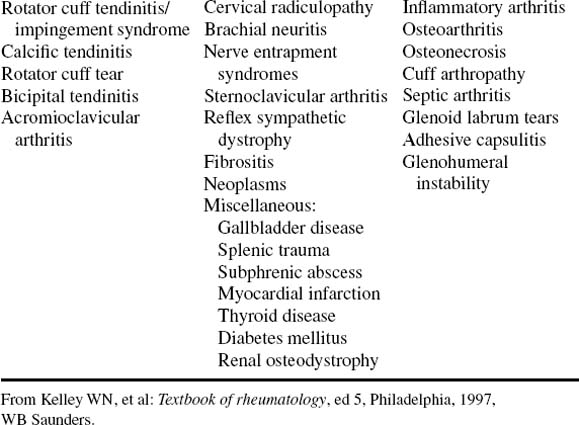
Referred pain to the shoulder can occur with cervical disorders, Pancoast tumor of the lung, a subphrenic pathologic condition, entrapment neuropathies, myofascial pain syndromes, and brachial neuritis (Table 4-3).
| Periarticular Disorders | Regional Disorders | Glenohumeral Disorders |
|---|---|---|
From Kelley WN, et al: Textbook of rheumatology, ed 5, Philadelphia, 1997, WB Saunders.
Identification of the primary cause of shoulder pain is not always easy. Referred pain to the shoulder girdle region occurs from multiple sources other than the neck. With diaphragmatic irritation, pain is referred along the phrenic nerve to the supraclavicular region, the trapezius, and the superomedial angle of the scapula. Gastric and pancreatic diseases may refer pain to the interscapular region. The rare superior sulcus lung tumor, or Pancoast tumor, occasionally coincident with Horner syndrome, may have shoulder pain as its initial symptom.
The mobility of this part of the body results from the configuration of the bony parts and the mechanically advantageous attachment of the multiple muscles. The shallow socket and ball head favor frictionless spinning, and the main joint has four accessory articulating zones that complement and enhance the action of the shoulder.
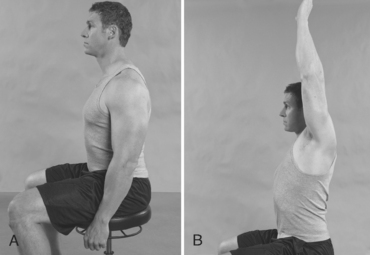
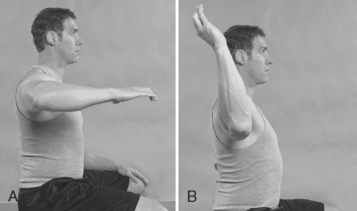
ESSENTIAL MOTION ASSESSMENT
Shoulder motion is interpreted through excursion of the arm from the body and is recorded according to the anatomic planes (Fig. 4-1).





ESSENTIAL MUSCLE FUNCTION ASSESSMENT
The teres major muscle arises from the lower third of the lateral border of the scapula and travels around the anterior aspect of the humerus and in front of the long head of the triceps to insert onto the crest of the lesser tubercle. The teres minor and deltoid receive their innervation by the axillary nerve, whereas the teres major is supplied by the lower subscapular nerve (Figs. 4-8 to 4-13).





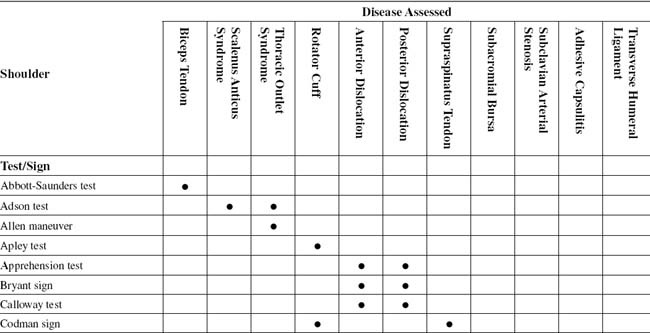
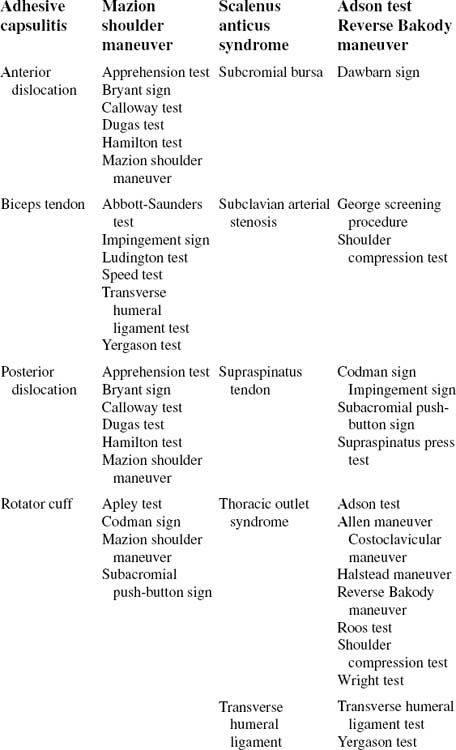
ABBOTT-SAUNDERS TEST
PROCEDURE

ADSON TEST (ALSO KNOWN AS SCALENE MANEUVER AND SCALENUS ANTICUS TEST)
PROCEDURE

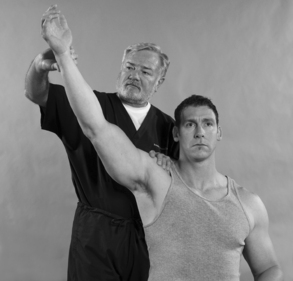
ALLEN MANEUVER
Assessment for Thoracic Outlet Syndrome
ORTHOPEDIC GAMUT 4-8 THORACIC OUTLET SYNDROME CLASSIFICATIONS
Thoracic outlet syndrome (TOS) is categorized in three types:
PROCEDURE
PROCEDURE


PROCEDURE


BRYANT SIGN
Assessment for Dislocation of the Glenohumeral Articulation
ORTHOPEDIC GAMUT 4-10 AXILLARY PSEUDOANEURYSM
PROCEDURE
The examiner views the characteristic lowering of the axillary fold (anterior and posterior pillars of the armpit) that is seen after trauma when dislocation of the glenohumeral articulation ensues (Fig. 4-21).

CODMAN SIGN (ALSO KNOWN AS DROP ARM TEST)
PROCEDURE

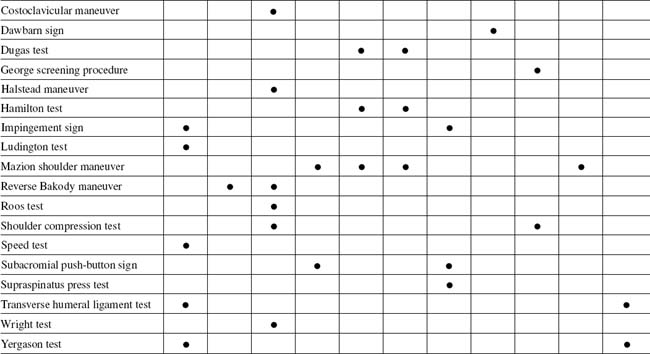
COSTOCLAVICULAR MANEUVER
Assessment for Thoracic Outlet Syndrome
ORTHOPEDIC GAMUT 4-13 SYMPTOMS OF SUBCLAVIAN VENOUS OBSTRUCTION


PROCEDURE

DUGAS TEST
PROCEDURE

GEORGE SCREENING PROCEDURE
PROCEDURE



HALSTEAD MANEUVER
PROCEDURE

HAMILTON TEST
PROCEDURE

IMPINGEMENT SIGN
Assessment for Overuse Injury to the Supraspinatus or Biceps Tendons
Comment
The terminology for impingement lesions had led to confusion. Many names and causes for this condition have been cited, including bursitis, tendinitis, acute trauma, overuse, instability, aging, tendon degeneration, vascular deficiencies, and mechanical impingement (Table 4-4). The rotator cuff is the only tendon situated between two bones.
TABLE 4-4 CLINICAL PRESENTATIONS OF THE MOST COMMON SHOULDER CONDITIONS
| Disorder | Age Group Affected | Key Diagnostic Features |
|---|---|---|
| Rotator cuff impingement | Middle-aged | Painful arc within full ROM |
| Rotator cuff tear | Middle-aged and older adults | Selective weakness of supraspinatus/infraspinatus |
| Frozen shoulder | Middle-aged | Restriction of passive ROM, external rotation |
| Calcific tendonitis | Middle-aged | Severe pain; full passive ROM; calcific deposit on radiograph |
| Acromioclavicular osteoarthosis | Middle-aged and older adults | Pain over joint; radiographic changes |
| Glenohumeral osteoarthosis | Middle-aged and older adults | Loss of passive ROM; radiographic changes |
| Shoulder instability | Age <40 years | Recurrent dislocation or subluxation symptoms; clinical signs of instability |
ROM, Range of motion.
Adapted from Frost A, Michael Robinson C: The painful shoulder, Surgery (Oxford) 24(11):363-367, 2006.

PROCEDURE

REVERSE BAKODY MANEUVER
Assessment for Cervical Foraminal Compression and Interscalene Compression
PROCEDURE

ROOS TEST
PROCEDURE

PROCEDURE

SUBACROMIAL PUSH-BUTTON SIGN (ALSO KNOWN AS MAZION CUFF MANEUVER)
Assessment for Rotator Cuff Tear of the Supraspinatus Tendon
Comment
Ruptures of the rotator cuff result from continued deterioration and degeneration (Table 4-5). The tear may be partial or complete.
TABLE 4-5 GOUTALLIER GRADING SYSTEM OF FATTY DEGENERATION OF MUSCLE
| Stage | Findings (MRI/CT) |
|---|---|
| Stage 0 | Normal muscle; no fatty streaking |
| Stage 1 | Occasional fatty streaking |
| Stage 2: fat < 50% of cross | Sectional area (fat < muscle) |
| Stage 3: fat = 50% of cross | Sectional area (fat = muscle) |
| Stage 4: fat > 50% of cross | Sectional area (fat > muscle) |
CT, Computed tomography; MRI, magnetic resonance imaging.
PROCEDURE

SUPRASPINATUS PRESS TEST
Assessment for Tear of the Supraspinatus Tendon or Muscle
ORTHOPEDIC GAMUT 4-28 SUPRASPINATUS SYNDROME
Variations of degeneration that lead to supraspinatus syndrome include the following:
PROCEDURE

PROCEDURE

WRIGHT TEST (ALSO KNOWN AS HYPERABDUCTION MANEUVER)
PROCEDURE
YERGASON TEST
Assessment for Tenosynovitis or Involvement of the Transverse Humeral Ligament
ORTHOPEDIC GAMUT 4-31 HAWKIN IMPINGEMENT TEST
For the Hawkin impingement test:
ORTHOPEDIC GAMUT 4-32 SUPRASPINATUS TEST: EMPTY CAN TEST

[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]
CHAPTER FOUR SHOULDER
AXIOMS IN ASSESSING THE SHOULDER
INTRODUCTION
Referred pain to the shoulder can occur with cervical disorders, Pancoast tumor of the lung, a subphrenic pathologic condition, entrapment neuropathies, myofascial pain syndromes, and brachial neuritis (Table 4-3).
| Periarticular Disorders | Regional Disorders | Glenohumeral Disorders |
|---|---|---|
From Kelley WN, et al: Textbook of rheumatology, ed 5, Philadelphia, 1997, WB Saunders.
Identification of the primary cause of shoulder pain is not always easy. Referred pain to the shoulder girdle region occurs from multiple sources other than the neck. With diaphragmatic irritation, pain is referred along the phrenic nerve to the supraclavicular region, the trapezius, and the superomedial angle of the scapula. Gastric and pancreatic diseases may refer pain to the interscapular region. The rare superior sulcus lung tumor, or Pancoast tumor, occasionally coincident with Horner syndrome, may have shoulder pain as its initial symptom.
The mobility of this part of the body results from the configuration of the bony parts and the mechanically advantageous attachment of the multiple muscles. The shallow socket and ball head favor frictionless spinning, and the main joint has four accessory articulating zones that complement and enhance the action of the shoulder.
ESSENTIAL MOTION ASSESSMENT
Shoulder motion is interpreted through excursion of the arm from the body and is recorded according to the anatomic planes (Fig. 4-1).
ESSENTIAL MUSCLE FUNCTION ASSESSMENT
The teres major muscle arises from the lower third of the lateral border of the scapula and travels around the anterior aspect of the humerus and in front of the long head of the triceps to insert onto the crest of the lesser tubercle. The teres minor and deltoid receive their innervation by the axillary nerve, whereas the teres major is supplied by the lower subscapular nerve (Figs. 4-8 to 4-13).
ABBOTT-SAUNDERS TEST
PROCEDURE
ADSON TEST (ALSO KNOWN AS SCALENE MANEUVER AND SCALENUS ANTICUS TEST)
PROCEDURE
ALLEN MANEUVER
Assessment for Thoracic Outlet Syndrome
ORTHOPEDIC GAMUT 4-8 THORACIC OUTLET SYNDROME CLASSIFICATIONS
Thoracic outlet syndrome (TOS) is categorized in three types:
PROCEDURE
PROCEDURE
PROCEDURE
[/not-level-membership-for-orthopaedics-category]
