Problem 48 Severe dehydration in a young woman
An 18-year-old girl is brought into the emergency department by ambulance from a youth hostel. She is a backpacker and has been travelling around the country. She is drowsy and unable to give any history. Her airway is clear and her breathing is unhindered. She reacts purposefully to painful stimuli, moving all limbs, and grunts but does not speak. She opens her eyes briefly in response to you shouting her name.
There are a number of possible causes for this woman’s comatose state.
You have a working diagnosis for this patient who is critically ill.
The patient decides to curtail her backpacking holiday and return home.
Answers
A.1 Her Glasgow coma score is 11 (E4, V2, M5).
A.3 As part of the immediate management, the following must be undertaken:
• Insert an intravenous cannula and take blood for electrolytes, urea and creatinine, blood glucose, complete blood picture, lipase.
• Commence emergency resuscitation with intravenous infusion of isotonic saline. At least 1–1.5 litres should be given over the first hour.
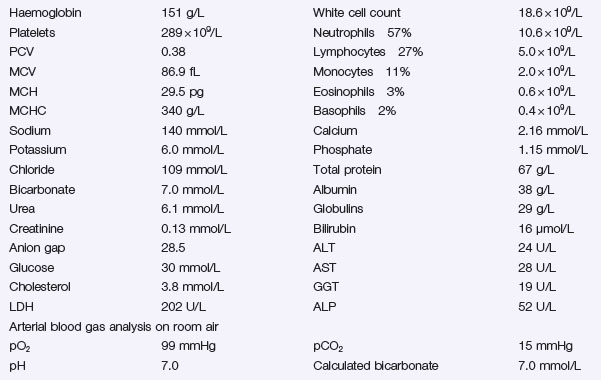
Metabolic acidosis can be divided into:
• High anion gap acidosis (addition of anions to the blood, e.g. ketoacidosis, lactic acidosis and salicylate or alcohol poisoning).
• Normal anion gap acidosis with a high chloride level, usually as a result of loss of alkali (bicarbonate), for example from the gut with severe diarrhoea or in renal tubular acidosis.
Fluid and Sodium Replacement
• Severe dehydration is common. This is secondary to the osmotic diuresis (hyperglycaemia and ketonuria) compounded by vomiting and hyperventilation. The degree of dehydration needs to be assessed both clinically and biochemically.
• Sodium depletion is common. This is consequent on the diuresis (although the serum sodium level may appear normal).
Correction of Acidosis and Hyperglycaemia with Insulin
Insulin therapy will correct both the acidosis and hyperglycaemia.
Potassium Replacement
• Replacement potassium can commence with the second litre of saline – provided the initial serum potassium was in the normal range.
• If the initial potassium level is high, recheck the potassium after 2 hours of intravenous saline infusion and commence potassium replacement as soon as the serum potassium is in the normal range (do not wait till hypokalaemia has occurred to start potassium replacement).
• Potassium replacement in range of 10–20 mmol/L/hour (1 g KCl = 13.6 mmol). This rate is likely to be required for the first 12 hours. Be prepared to increase this rate if serum potassium is not being maintained in the desirable range.
Prevention of the Complications of Ketoacidosis
• Cerebral oedema is a rare but dangerous complication; it can be prevented by careful fluid balance and avoiding dramatic drops in blood glucose levels.
• Aspiration of gastric contents can be prevented by careful nursing and keeping the patient fasting until she is fully conscious and has bowel sounds.
• Thrombosis is a relatively common complication; anticoagulation until the patient is mobile may need to be considered.
Insulin infusion is ceased 1 hour after the first dose of subcutaneous insulin is given.
In Hospital:
• She needs to be commenced on a basal/bolus insulin regimen using short-acting insulin before each main meal and basal insulin at bedtime. She should be taught the action of the different insulins that she will be using. (A starting dose of insulin may be estimated using the calculation of 0.3–0.5 unit insulin per kg of body weight per 24 hours split half into basal and half to be divided into the three bolus doses.)
• She needs to be taught to recognize the symptoms of hypoglycaemia and instructed on how to prevent and treat hypoglycaemia.
As an Outpatient
• A diet plan is important with basic knowledge on the appropriate food types. A balanced diet with complex carbohydrates should be encouraged and simple sugars avoided. The diet should have less than 30% as fat. Most importantly she should understand the necessity to eat regularly with an even spread of carbohydrates over the day and not to miss meals. Between-meal snacks and supper will need to be taken.
• She should be advised to be very moderate with alcohol consumption and to ensure that she eats adequate carbohydrate-type food when she drinks alcohol.
• She should be taught how to recognize the symptoms of hypoglycaemia and what the appropriate treatment is.
• She should be given information on how travelling can affect diabetes and what steps she needs to take.
• The patient needs to understand that diabetes is a lifelong disease that needs to be managed well to prevent long-term complications. However, details of long-term treatment and prevention and monitoring of long-term complications can be given at a later date when she is getting used to her condition.
Revision Points
Diabetic Ketoacidosis
• An increased need for insulin at times of physical stress (e.g. an intercurrent infection, trauma, surgery, etc.).
Treatment
Intravenous insulin infusion allows a gradual and steady correction of the metabolic abnormalities.