53 Seventh cranial nerve palsy
Lower motor neuron type
Salient features
History
• Onset: whether abrupt followed by worsening over the following day (Bell’s palsy)
• Pain over the preceding or accompanying the weakness (Bell’s palsy)
• The face itself feels stiff and pulled to one side
• Ipsilateral restriction of eye closure
• Disturbance of taste (caused by chorda tympani fibres)
• Hyperacusis (involvement of stapedius muscle in the inner ear).
Examination
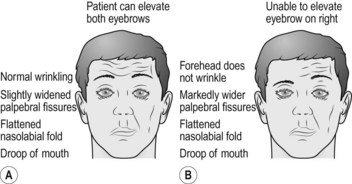
• Weakness of muscles of one half of the face; the patient is unable to screw his or her eyes tightly shut or move the angle of the mouth on the affected side (Fig. 53.1)
• Look for the following when the patient is unaware of being observed:
• Look at the external auditory meatus for herpes zoster (Ramsay Hunt syndrome)
• Look for parotid gland enlargement
• Examine for taste (loss of taste with the involvement of chorda tympani)
• Check for hearing (for hyperacusis resulting from involvement of the nerve to stapedius muscle)
• Examine tympanic membrane for otitis media
• Tell the examiner that you would like to test the urine for sugar (diabetes).
Questions
Advanced-level questions
What are the causes of bilateral facial nerve palsy?
What are causes of unilateral facial nerve palsy?
Lower motor neuron
All the muscles of one half of the face are affected:
• Bell’s palsy. Recent studies using a polymerase chain reaction (PCR) have implicated herpes simplex viral infection in Bell’s palsy. The incidence of Bell’s palsy is 23 per 100 000 individuals per year, or about 1 in 60–70 individuals per year. Men or women are affected equally and the peak incidence between the ages of 10 and 40. Both the right and left sides are affected with equal frequency
What do you know of nervus intermedius?
• Superior salivary nucleus (in the pons) supplies secretory fibres to the glands
• Gustatory or solitary nucleus (in the medulla) receives taste fibres via the chorda tympani
• Dorsal part of the trigeminal nerve receives cutaneous sensation from the external auditory meatus and the skin behind the ear (distributed with the facial nerve proper).
How would you manage Bell’s palsy?
• physiotherapy: massage, electrical stimulation, splint to prevent drooping of the lower part of the face
• protection of the eye with lubricating eye drops and a patch during sleep
• early treatment (within 72 h) with prednisolone significantly improves the chances of complete recovery at 3 and 9 months (N Engl J Med 2007;357:1598)
• aciclovir–prednisone is more effective in improving volitional muscle activity and in preventing partial nerve degeneration than placebo–prednisone treatment (Ann Otol Rhinol Laryngol 1996;105:371).
How would you localize facial nerve palsy?
• Involvement of the nuclei in the pons: associated ipsilateral sixth nerve palsy
• Cerebellopontine angle lesion: associated fifth and eighth nerve involvement
• Lesion in the bony canal: loss of taste (carried by the lingual nerve) and hyperacusis (caused by involvement of the nerve to stapedius).
Mention a few examples of facial synkinesis
• if fibres originally connected with muscles of the face later innervate the lacrimal gland, anomalous secretion of tears (crocodile tears) may occur while eating
• if fibres originally connected with the orbicularis oculi innervate the orbicularis oris, closure of the eyelids causes retraction of the mouth
• opening of the jaw may cause closure of the eyelids on the corresponding side (jaw-winking).
What parts of the facial nerve must be imaged when facial nerve palsy is suspected?
Both MRI and CT of the temporal bone are used when the facial nerve must be examined.
The following anatomic areas must be imaged when the facial nerve is studied:
Does the facial nerve communicate with other cranial nerves or cervical spinal nerves?
| Site | Communication |
|---|---|
| Internal acoustic meatus | Vestibulocochlear nerve |
| Geniculate ganglion | Splenopalatine nucleus, otic ganglion, sympathetic nerves around the middle meningeal artery |
| Facial canal | Auricular branche of the vagus nerve |
| Splenomastoid foramen | Glossopharnyngeal, vagus, great auricular, and auricular temporal nerves |
| Behind the ear | Lesser occipital nerve |
| On the face | Trigeminal |
| In the neck | Cutaneous cervical nerve |






