Segmental Left Ventricular Systolic Function
John C. Sciarra and Christopher J. Gallagher
Myocardial Segment Identification
Hear ye, hear ye. The Office of Homeland Security is not going to shoot me for revealing any state secrets here. You will need to know these segments and you will need to know which coronaries feed which walls and which segments.
I speak not with forked tongue.
This is a for sure on the test.
First, the whole thing, then we’ll back up and break it down.
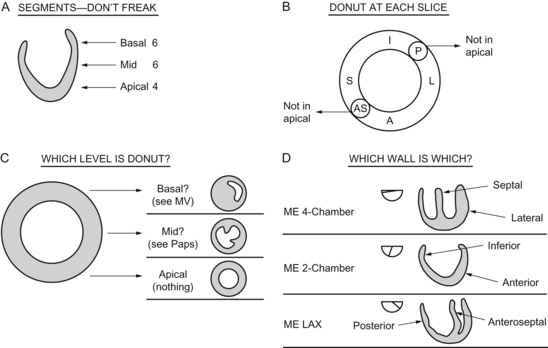
The basal 6 segments are next to the mitral valve.
The middle 6 segments are next down, at the level of the papillary muscles.
Coronary Artery Distribution and Flow
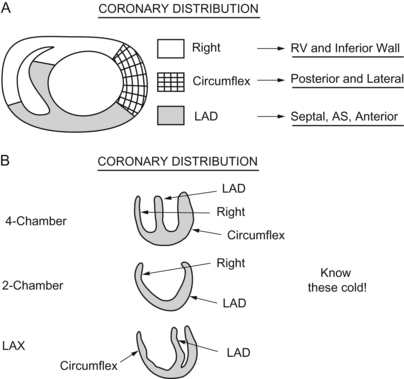
Let’s put it into words, just in case you’re less of a visual learner.
The right coronary feeds the inferior wall and right ventricle.
The circumflex feeds the posterior and lateral wall.
Here is a little memory helper I made up, I call it the “coronary artery memory helper”:
LM → LAD → Diags (the “D” in lad leads into the “D” in diagonals).
Circ → OMs (circumferential looks like the circumference of the “O” in Obtuse Marginal).
RC → PDA (the right hand [RCA] writes on the palm pilot pda).
Normal and Abnormal Segmental Dysfunction
Assessment and Methods
Keep your eyes open, that’s the method. The wall motion abnormalities you see will not be subtle. Every test-taker since the dawn of time emphasized that to me.
“You’ll see it moving, then BOOM, it ain’t moving.”




Differential Diagnosis






Confounding Factors
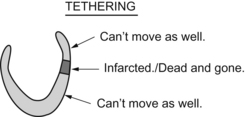
Tethering can throw you off the hunt when examining regional wall motion abnormalities.
Left Ventricular Aneurysm
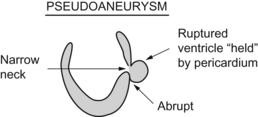
Of specific diagnostic interest, an aneurysm has a smooth transition from normal myocardium to thinned aneurysm. There is no sharp angle or neck (as we’ll see with pseudoaneurysms or ventricular ruptures in just a minute).
Questions
1. Regarding myocardial stunning:
A Ischemia tends to produce more severe wall motion abnormalities
B Stunned myocardium shows a gradual improvement and function in the first minutes to hours following separation from bypass
C Stunned myocardium may be recruited to contract with inotropic stimulation
D Inotropic stimulation may worsen function in an ischemic segment