92
Scabies
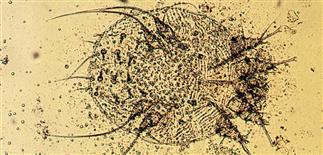
Sarcoptes scabiei mite in a potassium hydroxide wet mount (× 40). Even when scabies mites are present in the skin, it can be difficult to get a positive scabies prep.

Linear vesicle and burrows remain discrete, are characteristic and differentiate scabies from other vesicular diseases such as poison ivy.

Scabies mites like web spaces of the hands, feet and genital areas, causing red inflamed eczematous patches and burrows.

Secondary lesions, papules and nodules, may occur on the scrotum, penis, groin, axillae and buttocks. Mites may be absent from the lesions but pruritus persists, causing scratching and erosion of nodules.
DESCRIPTION
Intensely pruritic contagious human infestation caused by Sarcoptes scabiei var. hominis mite.
HISTORY
• Patients complain of unremitting itching (worst itch ever), cannot stop scratching. • Uncommon for scabies to present in just one family member. Other members, especially bed partners, also symptomatic. • Nodular lesions take longest to heal. • Crusted scabies (thousands of mites) may be source of epidemic scabies, may be seen in institutionalized and nursing home patients. • Persistent itching after adequate treatment due to a prolonged allergic response, presence of residual fecal matter and mite parts.
PHYSICAL FINDINGS
• Linear burrow is classic lesion. Burrow can be curved or S-shaped, slightly elevated. Inflamed vesicles and papules, 1–2 mm in size, also common features. May also present with scattered inflamed pustules, papules, and even larger nodules. • Individual lesions may be excoriated. • Typical locations are wrists, web spaces of hands, sides of hands and feet, genital area, warm intertriginous regions, abdomen. Scalp, palms, soles affected more often in infants. Secondary lesions (most common) have eczematous reaction pattern or secondary impetigo. Unique, advanced clinical variant is crusted (Norwegian) scabies. Patients—usually those with dementia, Down syndrome, immunosuppression—experience thick crusting and eczematous dermatitis, especially on hands, feet. Burrows most likely found in finger webs, wrists, sides of hands and feet, penis, buttocks, scrotum, and palms and soles of infants. • Can be misdiagnosed as insect bites, eczema, impetigo. • Mites, eggs, feces can be identified in a scabies preparation.
TREATMENT
• Apply permethrin (Elimite, Acticin) or lindane (Kwell) to entire skin surface from neck down, including under fingernails and toenails, and in umbilicus. Wash off in 8–12 h. • Head and neck uncommonly affected, but if lesions need treatment, take care to avoid eyes, mouth. Wash all clothes, bedclothes at time of application. House fumigation, extermination unnecessary. • Single dose of oral ivermectin (Stromectol, 6-mg scored tablet) (200 µg/kg) also safe and effective for most patients. Repeating dose 2 weeks later may provide higher cure rate. • Topical steroids may be used to control pruritus and inflammation after treatment with scabicide. Can treat persistent nodular lesions with intralesional steroids. • Can treat secondary bacterial infections with appropriate antibiotics. • Even adequately treated scabies may continue to itch for days to weeks after treatment, and does not need to be retreated in all cases.vn






