41 Saphenous Nerve Block
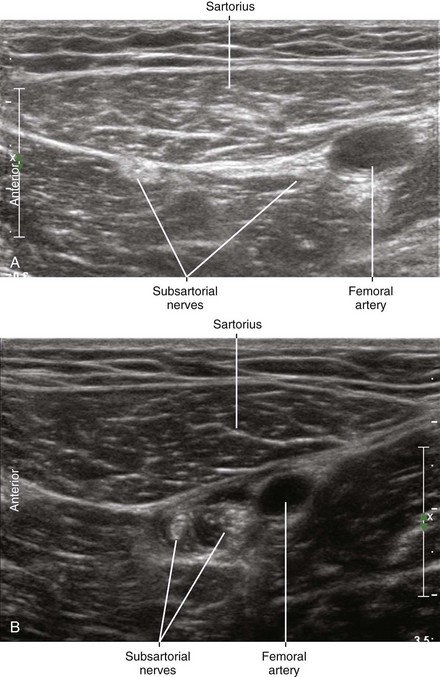
The saphenous nerve is a sensory branch of the femoral nerve that travels with the superficial femoral artery in the thigh along with the infrapatellar nerve and a nerve to the vastus medialis.1 Under the sartorius muscle, this complex forms the subsartorial plexus, which also can include contributions from the posterior division of the obturator nerve.2 The femoral artery and these nerves separate at the entrance to the adductor canal.3,4
The saphenous nerve emerges into the subcutaneous tissue between the sartorius and gracilis tendons within the pes anserinus to join the undersurface of the saphenous vein near the knee crease. The saphenous nerve and vein travel together in the leg to lie anterior to the medial malleolus. Saphenous nerve block is important for surgical anesthesia of the foot and ankle because it innervates the medial leg, malleolus, and foot. There are many approaches to saphenous nerve block along the course of the nerve.5
Suggested Technique
Subsartorial Plexus Block (Mid-Thigh)
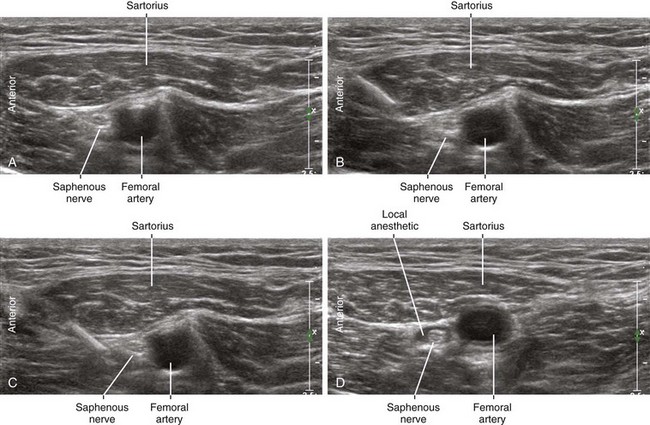
Saphenous nerve block can be performed in the mid-thigh with the patient in the supine position. An in-plane approach from the anterior thigh can be used to direct the needle tip through the sartorius muscle. The nerves of the subsartorial plexus can be imaged as a “bright triangle” anterior to the superficial femoral artery. The needle tip crosses the fascial plane on the anterior side of the nerves to avoid the neurovascular bundle. This subsartorial saphenous block is the deepest saphenous nerve block and therefore requires a steep angle of approach. However, the subsartorial plexus can often be directly imaged with ultrasound. The best access to the fascial layer of the nerves of the subsartorial plexus is usually attained by passing the block needle through the sartorius muscle rather than the vastus medialis. This trans-sartorial approach is similar to previous descriptions of saphenous nerve block that involved nerve stimulation.6
Vastoadductor Membrane Block (Distal Thigh)
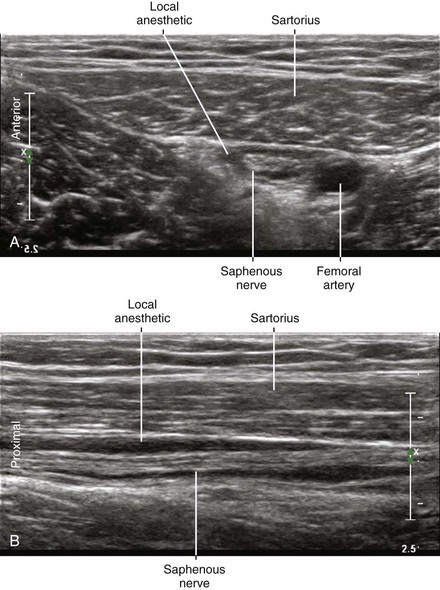
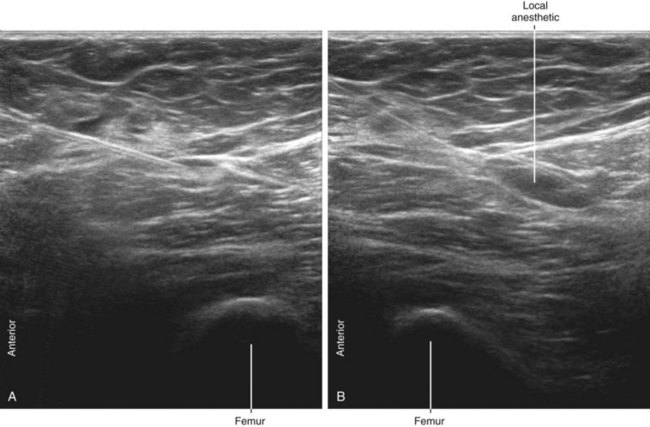
Saphenous nerve block also can be performed in the distal thigh with the patient in the supine position.7 An in-plane approach can be used to direct the needle tip through the vastus medialis just adjacent to the sartorius muscle. The muscles are viewed in short axis by placing the transducer on the distal aspect of the medial thigh with the needle introduced anteriorly. The local anesthetic injection should track within the fascial plane deep to the sartorius. Direct imaging of the saphenous nerve and the accompanying branch of the femoral artery is sometimes possible within this fascial plane.
Subcutaneous Infiltration Block (Proximal Leg)
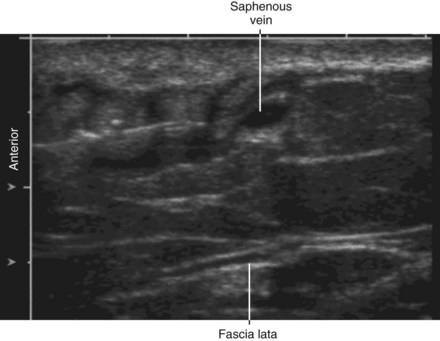
Saphenous nerve block can also be performed in the leg at the level of the tibial tuberosity.8 For this procedure, local anesthetic is infiltrated within the subcutaneous tissue near the saphenous vein using either an in-plane or out-of-plane approach. At this level the saphenous nerve and saphenous vein both lie superficial to the fascia lata. If the saphenous vein is difficult to visualize, a proximal tourniquet can be applied.
Key Points
| Saphenous Nerve Block | The Essentials |
|---|---|
| Anatomy | The SaN lies under the Sa anterior to the SFA. |
| Positioning | Supine, leg externally rotated and flexed at knee |
| Operator | Standing on the side of the patient |
| Display | Across the table |
| Transducer | High-frequency linear, 38- to 50-mm footprint |
| Initial depth setting | 35 mm |
| Needle | 20 to 21 gauge, 70 mm in length |
| Anatomic location | Mid-thigh, medial aspect |
| Approach | SAX view of SaN and Sa, in-plane from anterior to posterior |
| Place the needle tip through the Sa on the anterior side of the SFA. | |
| Sonographic assessment | The injection should track distally along the SaN under the Sa. |
| Anatomic variation | Position of the SaN and SFA can vary. |
Sa, Sartorius muscle; SaN, saphenous nerve; SAX, short axis; SFA, superficial femoral artery.
Clinical Pearls
• The saphenous nerve is a branch of the posterior division of the femoral nerve.
• The relation of the saphenous nerve to the femoral artery changes from lateral (near the inguinal region) to anterior (in the adductor canal).
• For the mid-thigh approach to saphenous nerve block, the sartorius muscle should be placed on the edge of the screen in short-axis view so that the block needle traverses this muscle for injection underneath it.
• This approach is similar to the subsartorial approach to saphenous nerve block.6
• Rotate the leg to improve the sartorial coverage of the saphenous nerve complex. This places the needle path through this muscle rather than the vastus medialis. Needle placement through the vastus medialis is more uncomfortable for the patient and more difficult for access to the fascial layers containing the nerves.
• After the injection under the sartorius muscle, slide the transducer over the known course of the saphenous nerve to verify the local anesthetic tracks along the branches of the subsartorial plexus.
• More distal block of the saphenous nerve is potentially more selective and carries less risk for vascular puncture. However, direct nerve imaging can be difficult with these distal approaches.



1 Thiranagama R. Nerve supply of the human vastus medialis muscle. J Anat. 1990;170:193–198.
2 Bouaziz H, Vial F, Jochum D, et al. An evaluation of the cutaneous distribution after obturator nerve block. Anesth Analg. 2002;94:445–449.
3 Scholten FG, Mali WP, Hillen B, et al. US location of the adductor canal hiatus: morphologic study. Radiology. 1989;172:75–78.
4 Tubbs RS, Loukas M, Shoja MM, et al. Anatomy and potential clinical significance of the vastoadductor membrane. Surg Radiol Anat. 2007;29:569–573.
5 Benzon HT, Sharma S, Calimaran A. Comparison of the different approaches to saphenous nerve block. Anesthesiology. 2005;102:633–638.
6 Mansour NY. Sub-sartorial saphenous nerve block with the aid of nerve stimulator. Reg Anesth. 1993;18:266–268.
7 Krombach J, Gray AT. Sonography for saphenous nerve block near the adductor canal. Reg Anesth Pain Med. 2007;32:369–370.
8 Gray AT, Collins AB. Ultrasound-guided saphenous nerve block. Reg Anesth Pain Med. 2003;28:148.