[level-membership-for-surgery-category]Chapter 36
Saphenofemoral Exposure

Femoral Anatomy
The femoral artery is an extension of the external iliac artery and by convention begins at the inguinal ligament. The first segment of the femoral artery and the femoral vein are enclosed within the femoral sheath and separated by a fiber septum (Fig. 36-1, A). The femoral sheath is a dense, fibrous band primarily consisting of two layers of fascia; the posterior aspect is a continuation of the fascia covering the pectineus muscle, and the anterior aspect is an extension of the transversalis fascia.
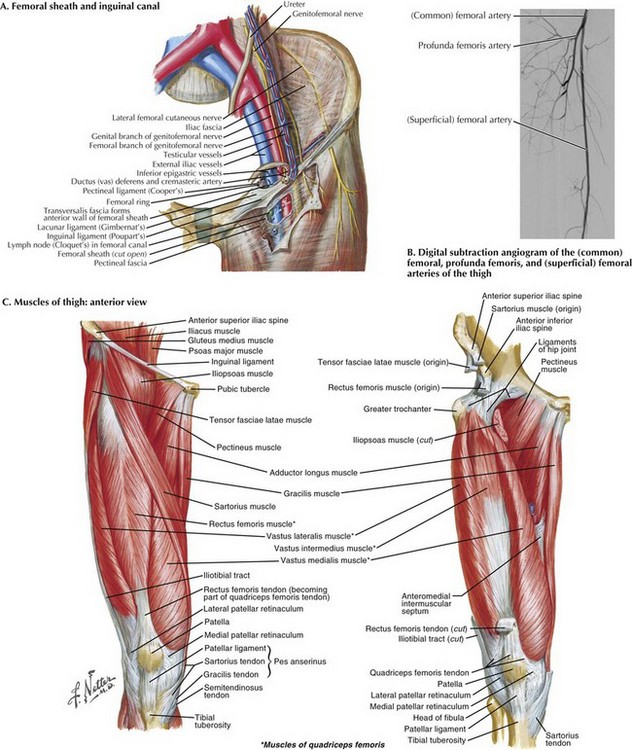
As the femoral artery moves obliquely over the pectineus muscle, it divides into two branches, the profunda femoris and superficial femoral (Fig. 36-1, B). The superficial femoral artery exits the femoral triangle into the subsartorial (Hunter’s) canal, crosses above the adductor longus muscle, and runs beneath the sartorius muscle (Fig. 36-1, C). As it moves distally, the superficial femoral artery decreases in caliber, eventually forming the popliteal artery.
Exposure of Femoral Artery
The most common approach allowing complete exposure of the common femoral artery and its branches is the vertical incision. The incision starts approximately at the midpoint of the inguinal ligament (Fig. 36-2, A). The patient is placed in the supine position. Location of the femoral pulse will guide the incision. Starting the incision directly over the pulse, 2 to 3 cm above the inguinal ligament, the surgeon continues the incision 4 to 8 cm distally toward the tip of the femoral triangle. In some cases, the patient’s pulse may not be palpable because of extensive calcification. If no pulse can be palpated, anatomic landmarks are identified: the pubic tubercle and anterior iliac spine (Fig. 36-2, B). The incision should be made at the midpoint between these two structures.
As the dissection deepens into the subcutaneous tissue, several small arteries (e.g., superficial epigastric, circumflex iliac) are encountered; these can be retracted or occasionally ligated and divided. Multiple lymph nodes and lymphatic channels lie within the path of dissection and should also be ligated and divided to avoid postoperative leak or lymphocele. Dissection is then continued through the fascia lata, exposing the medial margin of the sartorius muscle. With lateral retraction of the sartorius, the anterior lamella of the femoral sheath can be opened longitudinally with scissors or forceps to expose the femoral artery (Fig. 36-2, A). The lateral circumflex vein crosses over the origin of the profunda femoris and can be divided for adequate exposure of this artery.
An oblique incision is used where limited exposure of the femoral vessels is needed, as with endovascular device placement. The oblique approach is associated with lower wound morbidity than the standard vertical approach, including risk of infection and lymph leak. The patient is placed in the supine position and the inguinal ligament identified. Making an oblique incision approximately 2 to 2.5 fingerbreadths above the groin crease, the surgeon should make a cut in line with the inguinal ligament that runs over the palpated femoral pulse (Fig. 36-2, A). The incision is carried through the subcutaneous tissues to the fascia lata. Often, this is an avascular plane. All lymphatic tissue should be carefully ligated and divided to avoid a postoperative lymphocele. With the femoral sheath in view, it is then opened longitudinally, exposing the femoral artery.
Saphenofemoral Anatomy
The saphenofemoral junction is another important structure within the groin, located at the saphenous orifice (fossa ovalis) (Fig. 36-3, B). The saphenous opening is a small aperture in the fascia lata, inferior and lateral to the pubic tubercle and superior to the femoral vein. The fascia forms a curved edge lateral to the great saphenous vein. Its roof is composed of the cribriform fascia, the saphenous vein, and the venous tributaries that enter here.
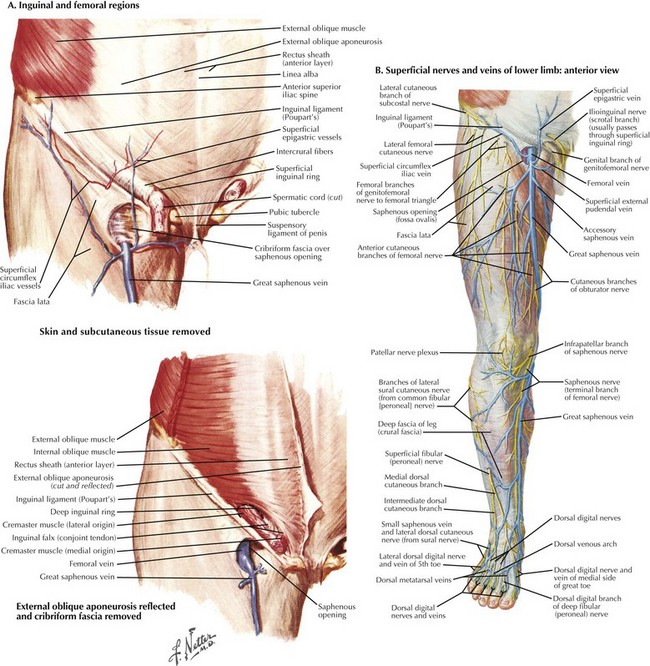
The great saphenous vein, common femoral vein, and the superficial inguinal veins join to form the saphenofemoral junction. Just before the fossa ovalis, multiple venous tributaries enter the great saphenous vein (e.g., superficial circumflex, superficial epigastric, lateral and medial accessory saphenous, external pudendal). Beginning at the superficial arch of the foot, the saphenous vein travels cephalad through the medial portion of the leg, above the deep fascia of the thigh, and then pierces the fascia of the femoral triangle, entering the fossa ovalis (Fig. 36-3, B).
Exposure of Saphenofemoral Junction
The great saphenous vein is found in the subcutaneous layer, coursing anteromedially along the thigh (Fig. 36-3, B).With the saphenous vein in view, the incision should be extended to the saphenofemoral junction (Fig. 36-3, A). The fascial covering of the trunk is dissected off the vein. Multiple tributaries enter the great saphenous vein, which then enters the fossa ovalis and joins the femoral vein. These venous tributaries can be ligated and divided. Identification of the external pudendal artery defines the lower border of the saphenofemoral opening.
Beirne, C, Martin, F, Hynes, N, Sultan, S. Five years’ experience of transverse groin incision for femoral artery access in arterial reconstructive surgery: parallel observational longitudinal group comparison study. Vascular. 2008;16(4):207–212.
Caiati, JM, Kaplan, D, Gitlitz, D, Hollier, LH, Marin, ML. The value of the oblique groin incision for femoral artery access during endovascular procedures. Ann Vasc Surg. 2000;14(3):248–253.
Schneider, DB, Sarkar, R, Messina, LM, Stoney, RJ. Extended iliac exposure from the groin. Vasc Surg. 2001;35(2):131–136.
Swinnen, J, Chao, A, Tiwari, A, et al. Vertical or transverse incisions for access to the femoral artery: a randomized control study. Ann Vasc Surg. 2010;24(3):336–341.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]Chapter 36
Saphenofemoral Exposure
Femoral Anatomy
The femoral artery is an extension of the external iliac artery and by convention begins at the inguinal ligament. The first segment of the femoral artery and the femoral vein are enclosed within the femoral sheath and separated by a fiber septum (Fig. 36-1, A). The femoral sheath is a dense, fibrous band primarily consisting of two layers of fascia; the posterior aspect is a continuation of the fascia covering the pectineus muscle, and the anterior aspect is an extension of the transversalis fascia.
As the femoral artery moves obliquely over the pectineus muscle, it divides into two branches, the profunda femoris and superficial femoral (Fig. 36-1, B). The superficial femoral artery exits the femoral triangle into the subsartorial (Hunter’s) canal, crosses above the adductor longus muscle, and runs beneath the sartorius muscle (Fig. 36-1, C). As it moves distally, the superficial femoral artery decreases in caliber, eventually forming the popliteal artery.
