[level-membership-for-pediatrics-category]
CHAPTER 35 Sacrococcygeal Teratoma
Step 1: Background and Surgical Anatomy


Step 2: Preoperative Considerations
Neonatal

Infant and Pediatric Patients
 Clinical assessment: A complete physical examination, including a digital rectal examination to evaluate the presacral region
Clinical assessment: A complete physical examination, including a digital rectal examination to evaluate the presacral region
 Radiologic studies: Generally ultrasound is adequate to delineate pelvic or abdominal extension. When a significant abdominal component is identified or concerns arise as to malignant potential, double-contrast computed tomography is useful to demonstrate the relation of the tumor to the rectum and urinary tract, as well as to exclude distant metastasis. Magnetic resonance imaging is particularly useful in evaluating anatomic relation to adjacent structures and possible infiltration into the spinal canal (Fig. 35-3).3
Radiologic studies: Generally ultrasound is adequate to delineate pelvic or abdominal extension. When a significant abdominal component is identified or concerns arise as to malignant potential, double-contrast computed tomography is useful to demonstrate the relation of the tumor to the rectum and urinary tract, as well as to exclude distant metastasis. Magnetic resonance imaging is particularly useful in evaluating anatomic relation to adjacent structures and possible infiltration into the spinal canal (Fig. 35-3).3


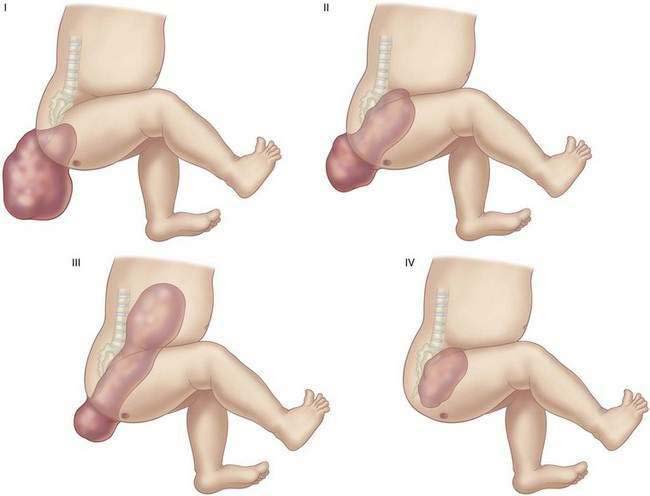
Table 35-1 Frequency of Malignancy Associated with Higher American Academy of Pediatrics Anatomic Classification
| AAP TYPE | MALIGNANT (%) | METASTASIS (%) |
|---|---|---|
| I | 8 | 0 |
| II | 21 | 6 |
| III | 34 | 20 |
| IV | 38 | 8 |
Step 3: Operative Steps
Positioning
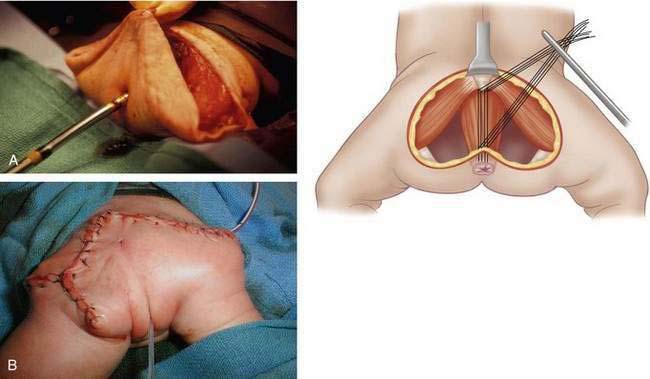
Operative Technique
Posterior Perineal Approach

Step 4: Postoperative Care




Step 5: Pearls and Pitfalls
1 Rescorla FJ, Sawin RS, Coran AG, et al. Long-term outcome for infants and children with sacrococcygeal teratoma: a report from the Childrens Cancer Group. J Pediatr Surg. 1998;33(2):171-176.
2 Rescorla FJ. Pediatric germ cell tumors. Semin Surg Oncol. 1999;16(2):144-158.
3 Skinner MA. Germ cell tumors. In: Keith T, Oldham PMC, Foglia RP, Skinner MA, editors. Principles and practice of pediatric surgery, vol. 1. Lippincott Williams & Wilkins; 2005:637-648.
4 Altman RP, Randolph JG, Lilly JR. Sacrococcygeal teratoma: American Academy of Pediatrics Surgical Section Survey-1973. J Pediatr Surg. 1974;9(3):389-398.
5 Rescorla F, Billmire D, Stolar C, et al. The effect of cisplatin dose and surgical resection in children with malignant germ cell tumors at the sacrococcygeal region: a pediatric intergroup trial (POG 9049/CCG 8882). J Pediatr Surg. 2001;36(1):12-17.
6 Currarino G, Coln D, Votteler T. Triad of anorectal, sacral, and presacral anomalies. AJR Am J Roentgenol. 1981;137(2):395-398.
7 Boemers TM, van Gool JD, de Jong TP, Bax KM. Lower urinary tract dysfunction in children with benign sacrococcygeal teratoma. J Urol. 1994;151(1):174-176.
[/level-membership-for-pediatrics-category][not-level-membership-for-pediatrics-category]
CHAPTER 35 Sacrococcygeal Teratoma
Step 1: Background and Surgical Anatomy
Step 2: Preoperative Considerations
Neonatal
Infant and Pediatric Patients
Clinical assessment: A complete physical examination, including a digital rectal examination to evaluate the presacral region Radiologic studies: Generally ultrasound is adequate to delineate pelvic or abdominal extension. When a significant abdominal component is identified or concerns arise as to malignant potential, double-contrast computed tomography is useful to demonstrate the relation of the tumor to the rectum and urinary tract, as well as to exclude distant metastasis. Magnetic resonance imaging is particularly useful in evaluating anatomic relation to adjacent structures and possible infiltration into the spinal canal (Fig. 35-3).3Table 35-1 Frequency of Malignancy Associated with Higher American Academy of Pediatrics Anatomic Classification
[/not-level-membership-for-pediatrics-category]
