Chapter 15 Rotational and Free Flap Closure of the Abdominal Wall 
1 Preoperative Considerations
1 Comorbidities









3 Timing









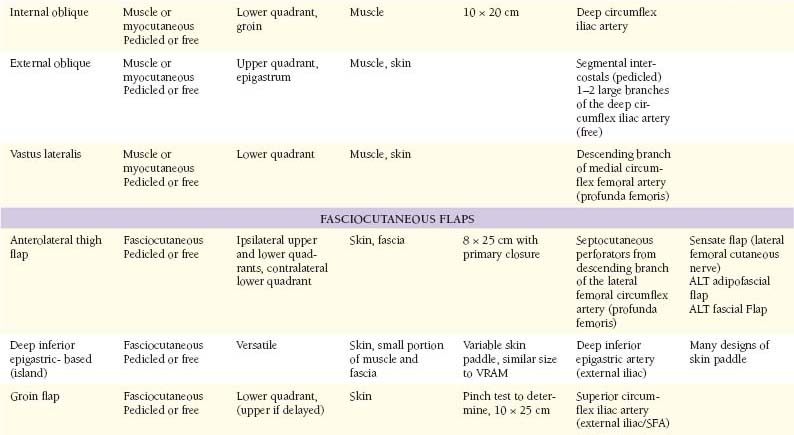
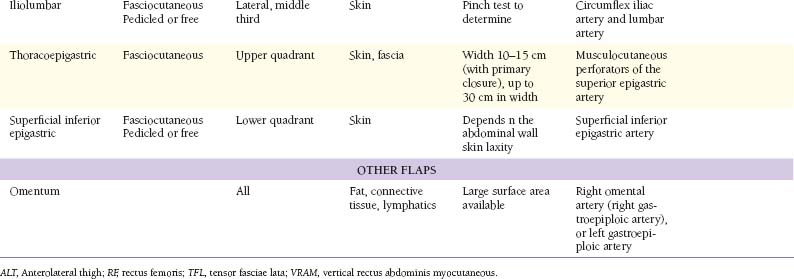
2 Muscular Flaps (Table 15-1)
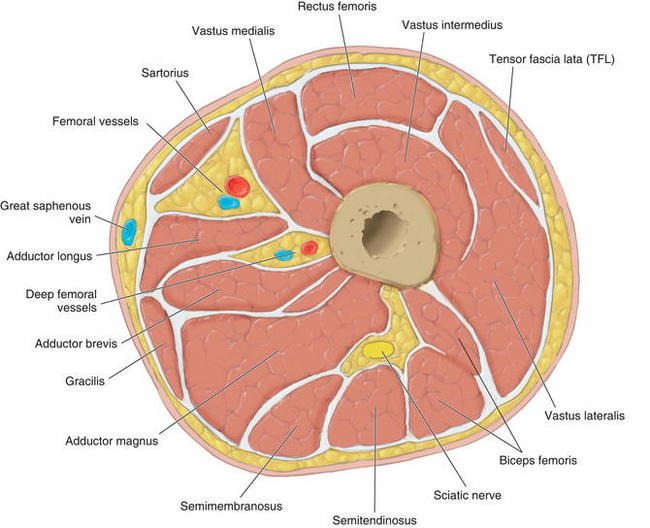
 Figure 15-1 shows the cross-sectional anatomy of the thigh demonstrating the possible muscles for coverage of abdominal wall defects
Figure 15-1 shows the cross-sectional anatomy of the thigh demonstrating the possible muscles for coverage of abdominal wall defects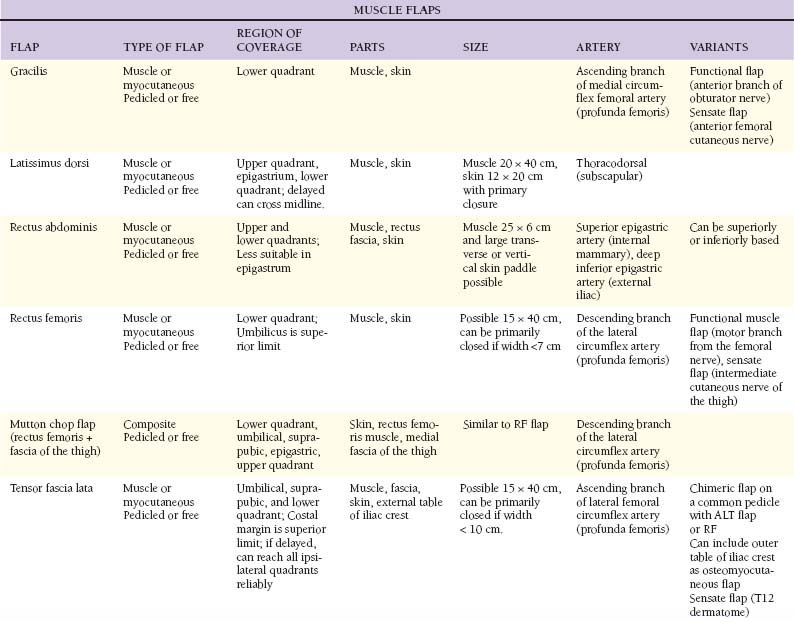
1 Tensor fascia lata
 Anatomy
Anatomy




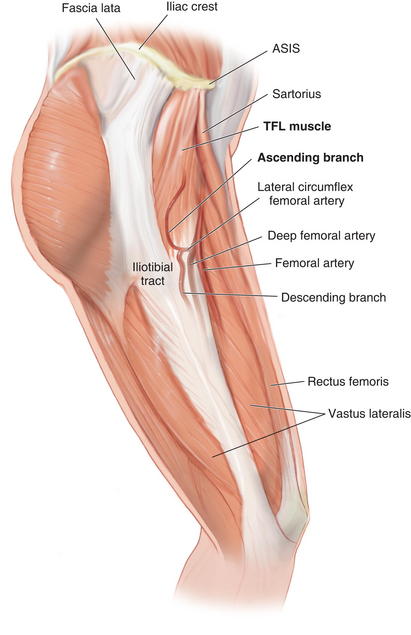
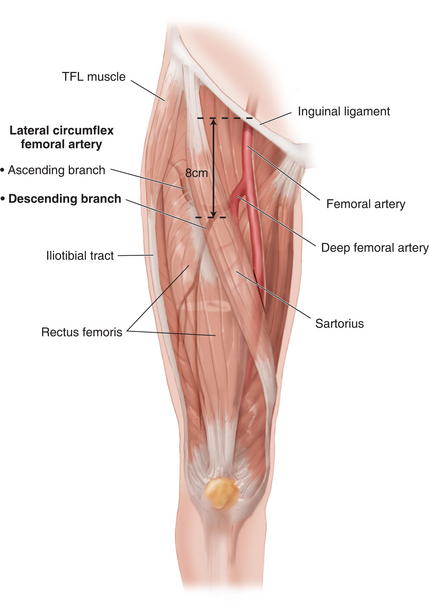
 The descending branch of the lateral femoral circumflex artery continues beyond the TFL muscle to supply the skin of the anterolateral midthigh and the lower thigh. It can be harvested with the anterolateral thigh skin to enlarge the perfused vascular territory.
The descending branch of the lateral femoral circumflex artery continues beyond the TFL muscle to supply the skin of the anterolateral midthigh and the lower thigh. It can be harvested with the anterolateral thigh skin to enlarge the perfused vascular territory. The TFL muscle (Fig. 15-2) is a short, flat muscle that is approximately 12 to 15 cm long. It acts as an accessory flexor and medial rotator of the thigh. It originates from the anterior iliac crest and the deep surface of the fascia lata. At the origin, it lies between the gluteus medius and sartorius, and superficial to the vastus lateralis. It inserts into the iliotibial tract, which inserts distally on Gerdy’s tubercle on the lateral aspect of the tibia.
The TFL muscle (Fig. 15-2) is a short, flat muscle that is approximately 12 to 15 cm long. It acts as an accessory flexor and medial rotator of the thigh. It originates from the anterior iliac crest and the deep surface of the fascia lata. At the origin, it lies between the gluteus medius and sartorius, and superficial to the vastus lateralis. It inserts into the iliotibial tract, which inserts distally on Gerdy’s tubercle on the lateral aspect of the tibia.
 Flap Design
Flap Design
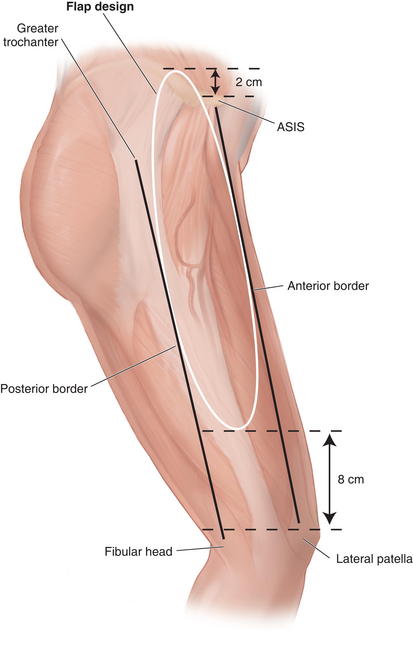
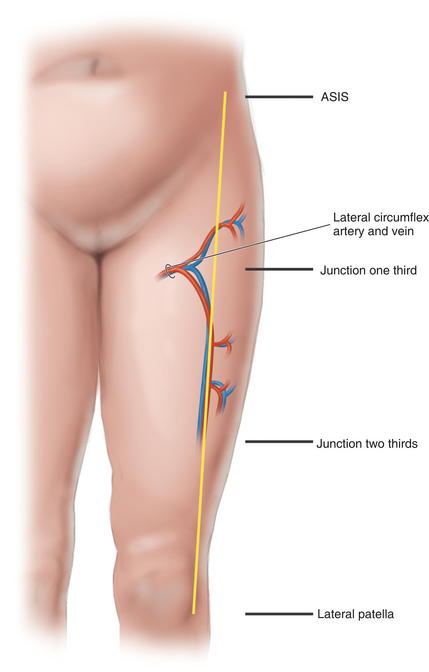
 Skin territory can be up to 15 × 40 cm. A line from the ASIS 10 to 15 cm posteriorly marks the origin of the TFL muscle, with the skin territory extending 2 cm cranial to this line (Fig. 15-3). The lower skin territory is 8 cm above the lateral femoral condyle. Posterior skin territory is a line drawn from the greater trochanter to the fibular head or approximately along the axis of the femur. The anterior border is a line drawn from the ASIS to the lateral aspect of the patella.
Skin territory can be up to 15 × 40 cm. A line from the ASIS 10 to 15 cm posteriorly marks the origin of the TFL muscle, with the skin territory extending 2 cm cranial to this line (Fig. 15-3). The lower skin territory is 8 cm above the lateral femoral condyle. Posterior skin territory is a line drawn from the greater trochanter to the fibular head or approximately along the axis of the femur. The anterior border is a line drawn from the ASIS to the lateral aspect of the patella.

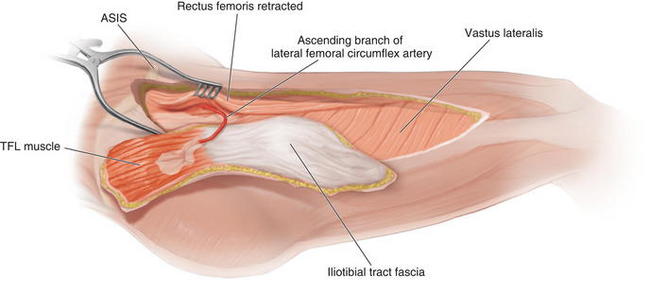
 Marking and Dissection
Marking and Dissection




















2 Latissimus dorsi




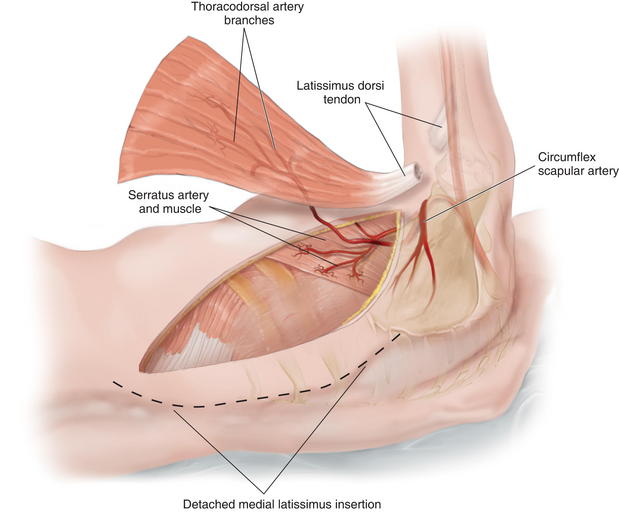
 Blood Supply
Blood Supply
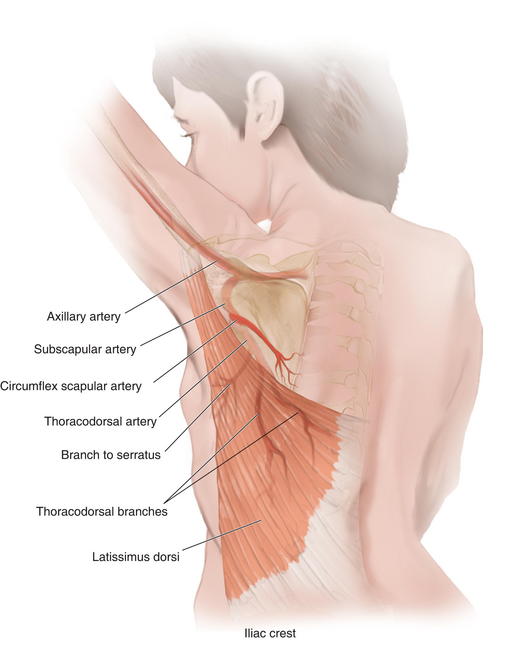
 Arterial blood is supplied through a terminal branch of the subscapular artery (2 to 5 mm diameter), a branch of the axillary artery.
Arterial blood is supplied through a terminal branch of the subscapular artery (2 to 5 mm diameter), a branch of the axillary artery.







 Flap Design
Flap Design
 The flap design can cover ipsilateral abdominal defects. If raised as an “extended” variant, it can cross the midline by incorporating the rim of supragluteal fascia.
The flap design can cover ipsilateral abdominal defects. If raised as an “extended” variant, it can cross the midline by incorporating the rim of supragluteal fascia.




 Marking and Dissection
Marking and Dissection
 The outline of the anterior and superior edges of the muscle is made. This can be facilitated by having the patient contract the latissimus.
The outline of the anterior and superior edges of the muscle is made. This can be facilitated by having the patient contract the latissimus.























3 Rectus Femoris
 Anatomy
Anatomy
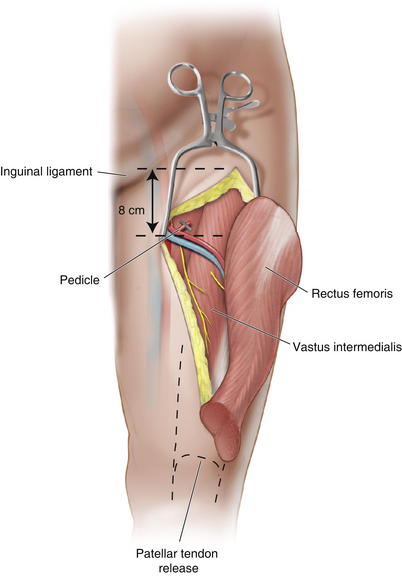
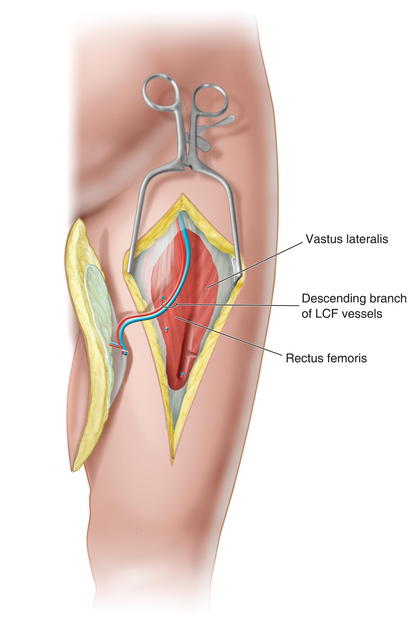
 Blood supply: The descending branch of the lateral circumflex artery (1.5 to 2 mm diameter) (Fig. 15-7) from the profunda femoris is located 8 cm below the inguinal ligament and enters the muscle on its deep surface. It also supplies the tissue of the anterolateral thigh flap.
Blood supply: The descending branch of the lateral circumflex artery (1.5 to 2 mm diameter) (Fig. 15-7) from the profunda femoris is located 8 cm below the inguinal ligament and enters the muscle on its deep surface. It also supplies the tissue of the anterolateral thigh flap.












 Marking and Dissection
Marking and Dissection
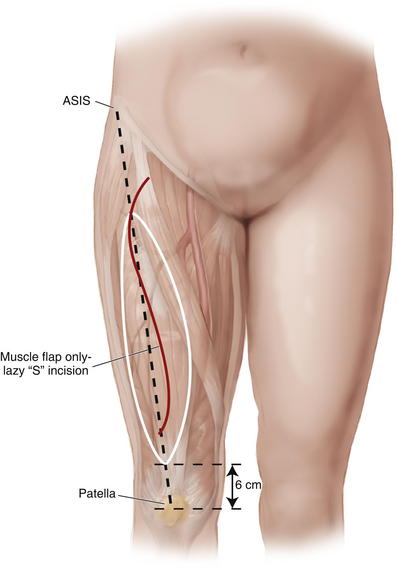
 The muscle falls on a line drawn from the ASIS to the middle aspect of the patella and terminates approximately 6 cm superior to the patella (Fig. 15-8).
The muscle falls on a line drawn from the ASIS to the middle aspect of the patella and terminates approximately 6 cm superior to the patella (Fig. 15-8).




















3 Fasciocutaneous Flaps (Fig. 15-10, see Table 15-1)
 Many flaps can be created in the trunk and torso. As depicted in Figure 15-10, on the right side of the torso are axially based flaps, including the deltopectoral, thoracoepigastric, groin, and hypogastric flaps. On the left side of the torso are depictions of bipedicled and laterally based cutaneous flaps.
Many flaps can be created in the trunk and torso. As depicted in Figure 15-10, on the right side of the torso are axially based flaps, including the deltopectoral, thoracoepigastric, groin, and hypogastric flaps. On the left side of the torso are depictions of bipedicled and laterally based cutaneous flaps.
1 Groin flap
 Anatomy
Anatomy
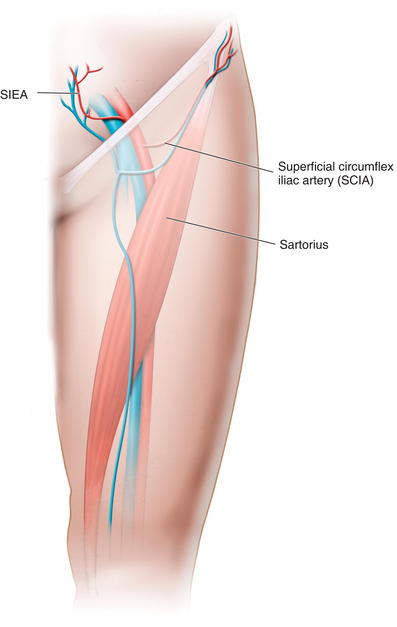
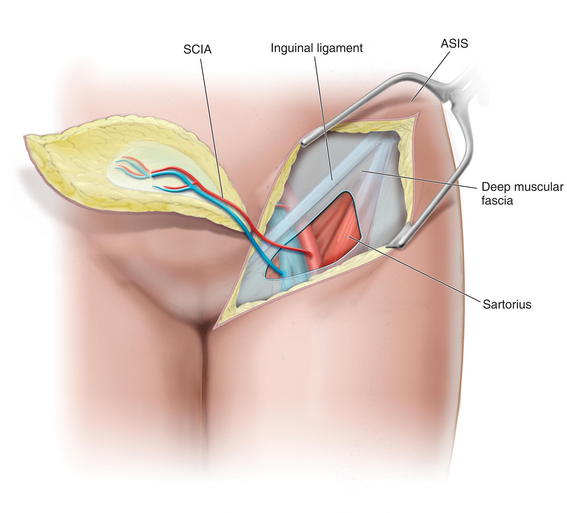
 Blood is supplied by the superficial circumflex iliac artery (SCIA) from the external iliac/superficial femoral artery at the level of the inguinal ligament (Fig. 15-11). The artery may arise directly from the femoral vessel or from the trunk of a parent vessel supplying the SCIA and the deep circumflex iliac artery (DCIA). The artery also can arise from a common trunk that gives off the superficial inferior epigastric artery (SIEA).
Blood is supplied by the superficial circumflex iliac artery (SCIA) from the external iliac/superficial femoral artery at the level of the inguinal ligament (Fig. 15-11). The artery may arise directly from the femoral vessel or from the trunk of a parent vessel supplying the SCIA and the deep circumflex iliac artery (DCIA). The artery also can arise from a common trunk that gives off the superficial inferior epigastric artery (SIEA).
























2 Extended Deep Inferior Epigastric Perforator Flap
 Anatomy
Anatomy
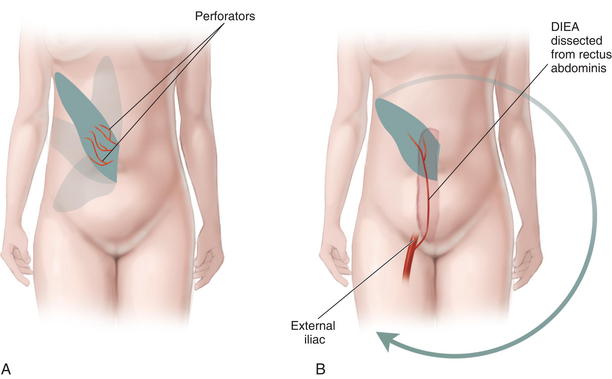
 The course and connections of the deep inferior epigastric artery (DIEA) have been previously covered.
The course and connections of the deep inferior epigastric artery (DIEA) have been previously covered.









 Markings and Dissection
Markings and Dissection
 The markings are determined by the defect, with the length of the pedicle obtainable; many variations of shape and size are possible, as long as perforators are included.
The markings are determined by the defect, with the length of the pedicle obtainable; many variations of shape and size are possible, as long as perforators are included.










3 Thoracoepigastric Flap
 Anatomy
Anatomy
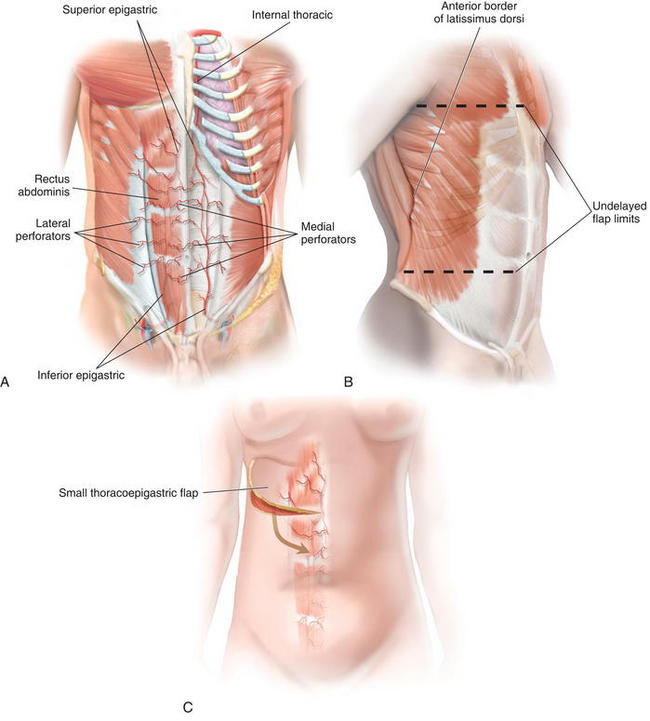
 The DIEA supplies the majority of the major perforating vessels leaving the rectus abdominis muscle and running laterally to the area of the latissimus in a suprafascial plane.
The DIEA supplies the majority of the major perforating vessels leaving the rectus abdominis muscle and running laterally to the area of the latissimus in a suprafascial plane.

 Flap Design
Flap Design


















4 Anterolateral Thigh





 Flap Design
Flap Design


 Marking and Dissection
Marking and Dissection
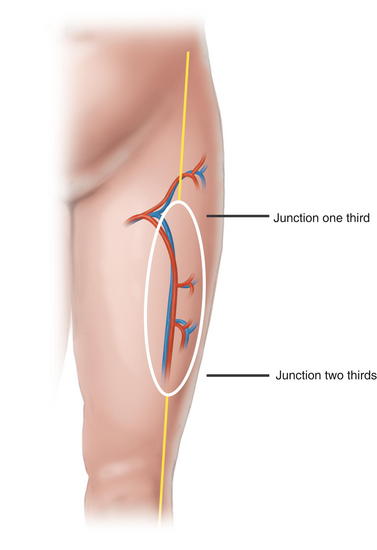
 The axis of the septum between the rectus femoris and the vastus lateralis is marked by a line connecting the ASIS and the lateral patella (Fig. 15-15).
The axis of the septum between the rectus femoris and the vastus lateralis is marked by a line connecting the ASIS and the lateral patella (Fig. 15-15).
 The junction of the middle and distal third is marked and is also incorporated into the flap (Fig. 15-16).
The junction of the middle and distal third is marked and is also incorporated into the flap (Fig. 15-16).













4 Postoperative Care











Gottlieb J.R., Engrav L.H., Walkinshaw M.D., Eddy A.C., Herman C.M. Upper abdominal wall defects: immediate or staged reconstruction? Plast Reconstr Surg. 1990;86(2):281-286.
Mansberger A.R.Jr., Kang J.S., Beebe H.G., Le Flore I. Repair of massive acute abdominal wall defects. J Trauma. 1973;13(9):766-774.
Mathes S.J., Steinwald P.M., Foster R.D., Hoffman W.Y., Anthony J.P. Complex abdominal wall reconstruction: a comparison of flap and mesh closure. Ann Surg. 2000;232(4):586-596.
Rohrich RJ, Lowe JB, Hackney FL, Bowman JL, Hobar PC: An algorithm for abdominal wall reconstruction. Plast Recon Surg 105(1): 202–216.
Steinwald P.M., Mathes S.J. Management of the complex abdominal wall wound. Adv Surg. 2001;35:77-108.
Strauch B., Vasconez L.O., Hall-Findlay E.J., editors. Grabb’s Encyclopedia of Flaps, ed 2, Philadelphia: Lippincott- Raven, 1998.
Yeh K., Saltz R., Howdieshell T. Abdominal wall reconstruction after temporary abdominal wall closure in trauma patients. Southern Medical Journal. 1996;89(5):497-502.
