[level-membership-for-cardiothoracic-surgery-category]
CHAPTER 8 Right Upper Lobectomy—video 8
Approach to Video-Assisted Right Upper Lobectomy
Order of Operative Steps
The order of the steps of the operation is as follows: level 10 nodes, RUL vein, anterior trunk of the pulmonary artery, minor fissure, posterior ascending artery, RUL bronchus, and the remainder of the fissure. The incisions are the standard incisions, with the utility incision placed directly up (lateral) from the superior pulmonary vein (see Chapter 1).
Key Points
 Video-Assisted Right Upper Lobectomy (Video 8-1)
Video-Assisted Right Upper Lobectomy (Video 8-1)
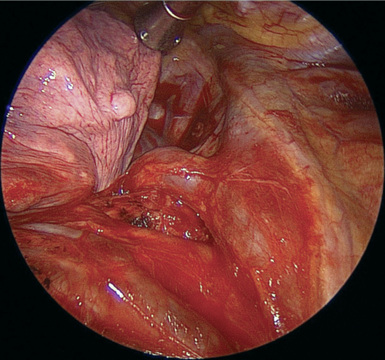
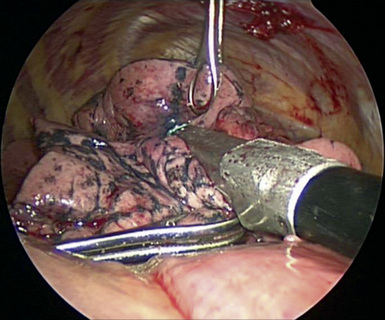
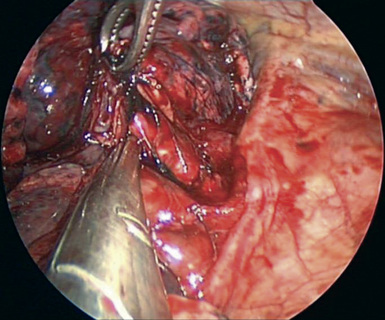
Step 1. Level 10 Nodes
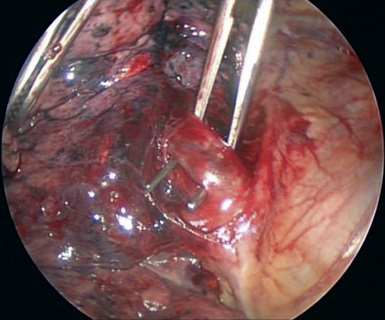
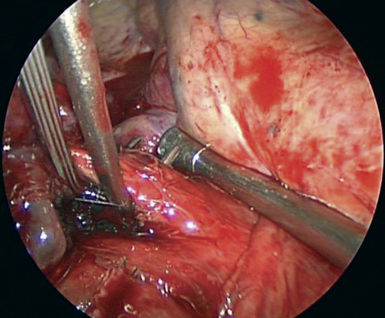
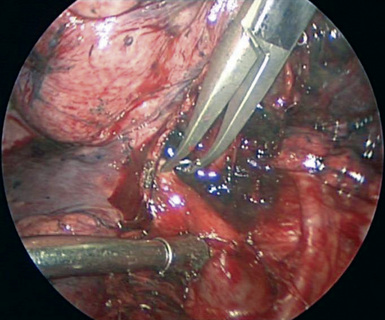
Step 2. Right Upper Lobe Vein
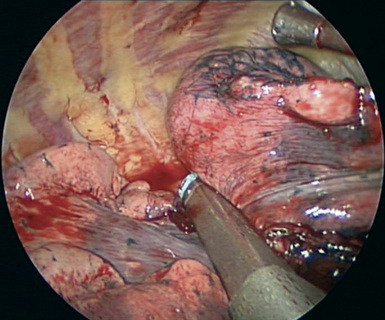
Step 3. Minor Fissure
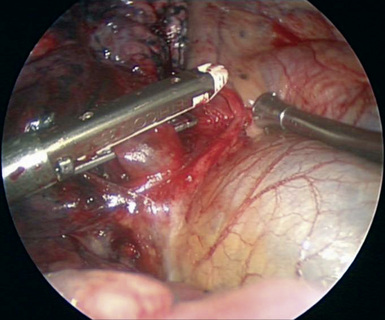
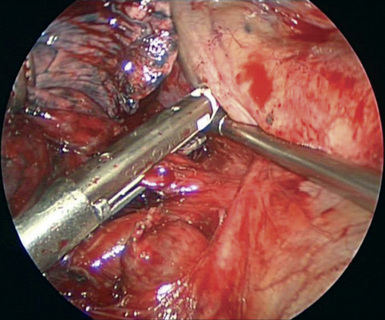
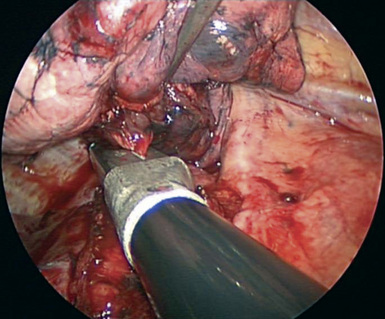
Step 4. Anterior Trunk
Step 5. Define Right Upper Lobe Bronchus
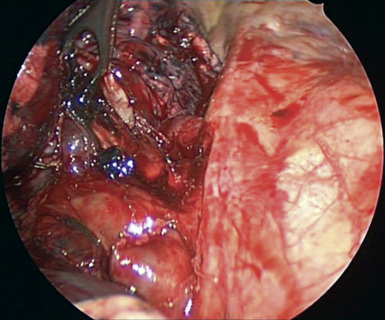
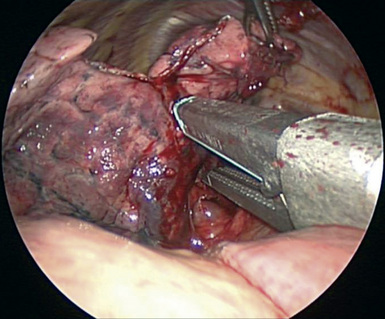
Step 6. Posterior Ascending Artery
Step 7. Right Upper Lobe Bronchus
Step 9. Lobe Removal
[/level-membership-for-cardiothoracic-surgery-category][not-level-membership-for-cardiothoracic-surgery-category]
CHAPTER 8 Right Upper Lobectomy—video 8
Approach to Video-Assisted Right Upper Lobectomy
Order of Operative Steps
The order of the steps of the operation is as follows: level 10 nodes, RUL vein, anterior trunk of the pulmonary artery, minor fissure, posterior ascending artery, RUL bronchus, and the remainder of the fissure. The incisions are the standard incisions, with the utility incision placed directly up (lateral) from the superior pulmonary vein (see Chapter 1).
Key Points
Video-Assisted Right Upper Lobectomy (Video 8-1)
Step 1. Level 10 Nodes
Step 2. Right Upper Lobe Vein
[/not-level-membership-for-cardiothoracic-surgery-category]
