8 Rheumatology
Osteoarthritis (OA)
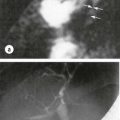
Describe the main radiological features of OA of the hip
The radiograph shows joint space narrowing, periarticular sclerosis, cyst formation and osteophytes. These are the four classic features of osteoarthritis (Fig. 8.1).
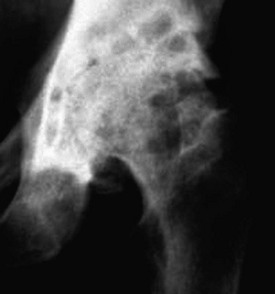
How would you assess this patient?
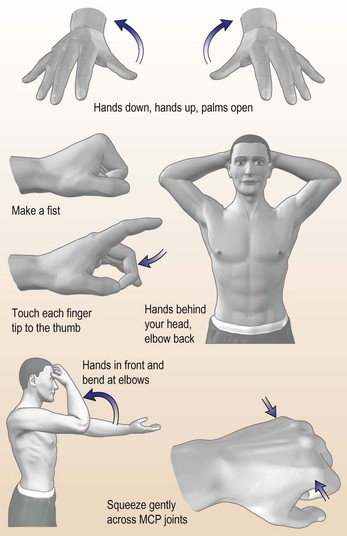
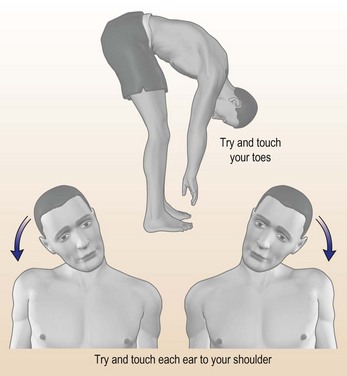
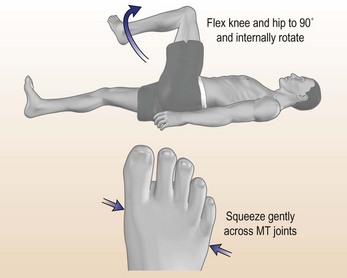
A full musculoskeletal examination is needed. The GALS (Gait, Arms, Leg, Spine) is a useful screen (Doherty et al., 1992) (Fig. 8.2).
Diagnostic clues
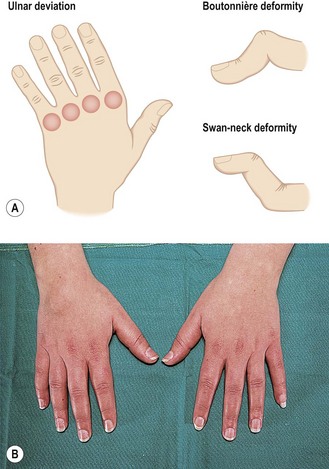
Look for Heberden’s (distal interphalangeal joints)/Bouchard’s (proximal) nodes, ‘square’ hands, painful thumb, carpometacarpal joints that indicate primary nodal OA. Figure 8.3 shows the distributions of generalised OA and pyrophosphate arthropathy.

Examine
Initial treatment
• Analgesia: simple or compound analgesia as first-line therapy, e.g. paracetamol up to 4 g/day. If this fails, a short course of an NSAID, e.g. Diclofenac usually helps the pain. There is a high risk of GI toxicity with long-term NSAID use in her age group. A gastro-cytoprotective agent, e.g. omeprazole, should be co-prescribed. Opiates should be avoided unless other analgesia has not worked because of sedation/confusion and constipation.
Later management
Refer to rheumatologist or medicine for the elderly consultant. In the meantime, organise:
There should be detailed planning before discharge, including liaison with the doctor and a home visit.
Rheumatoid arthritis (RA)
What other conditions could give a similar clinical picture?
In the first two differential diagnoses there are often other features. In SLE photosensitive rashes, hair loss, serositis and oral ulceration are seen. Erythrovirus B19 nearly always presents with flu-like symptoms and a widespread rash.
How would you manage this patient?
A full history and general medical examination is essential. Specific points:
• Look for nodules or vasculitis: uncommon at first presentation.
• A full musculoskeletal examination noting the symmetry of the joint involvement.
• Look for persistent inflammatory symmetrical arthritis (PISA). The most common cause of this is rheumatoid arthritis.
The most commonly involved joints at onset in rheumatoid arthritis are: wrists, MCPs, PIPs and MTP joints.
Admission is necessary if the patient is very unwell systemically and to exclude other pathology.

Initial management
• A short period of bed rest, ice packs if only a few joints involved.
• NSAIDS: ibuprofen is the safest; other NSAIDs have a higher risk of GI toxicity, although this patient is young.
• Disease-modifying anti-rheumatic drugs (DMARDs): these should be given at the earliest opportunity because RA is a systemic disease that leads rapidly to joint damage and disability. It is no longer acceptable to treat RA with NSAIDs alone. There is accumulating evidence to show that early DMARD use delays joint damage and functional disability.
Initial DMARDs commonly used include sulfasalazine, methotrexate or azathioprine. Others, such as IM gold and D-penicillamine, are less commonly used but still effective. Hydroxychloroquine and auranofin are the least effective but can be used in combination regimens. Combination therapies are showing good results.
SLE and vasculitis
Discuss the differential diagnosis, investigation and management
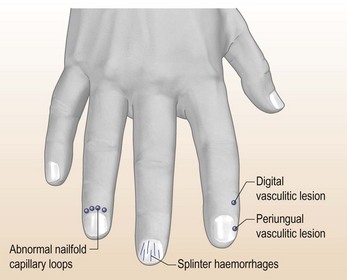
The differential diagnosis includes an inflammatory autoimmune rheumatic disease such as systemic lupus erythematosus (SLE), which has developed after delivery of her baby. The lesions on her hands (Fig. 8.6) and feet are strongly suggestive of vasculitis, which is a serious prognostic factor that requires immediate therapy.
Investigations (Table 8.1) are performed to look for the possibility of major organ involvement, which might be vasculitic. Her urine must be tested immediately for blood and protein and sent for urine cytology looking for fragmented red cells and/or casts. The presence of an ‘active’ urine sediment with fragmented or dysmorphic red cells and granular casts has a > 90% specificity for glomerulonephritis.
| Investigation | Typical finding |
|---|---|
| FBC | Immune cytopenias, especially neutropenia and thrombocytopenia, are common in SLE |
| There may be anaemia of chronic disease or haemolytic anaemia – check Coombs’ test. | |
| ESR and CRP | The pattern of a high ESR but normal CRP is characteristic of SLE |
| Renal function | U&E, 24-h urine protein/eGFR |
| Liver biochemistry | Hypoalbuminaemia is common |
| Lupus serology | |
| ANA | Present in 95% of SLE patients |
| dsDNA | Specific marker for SLE. A negative dsDNA, however, does not exclude SLE |
| ENA | Ro/La photosensitivity/Sjogren’s RNP/Sm often seen in severe SLE |
| Complement | Low values indicate activation of complement or rarely congenital deficiency |
| ANCA | A marker of vasculitis: a systemic vasculitis is an alternative to SLE |
Acute autoimmune rheumatic disease
What is the likely diagnosis?
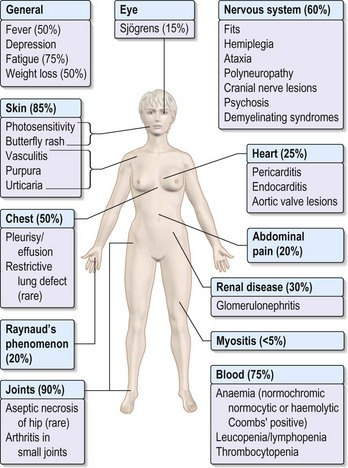
This patient has many characteristic features of SLE: inflammatory polyarthritis, mouth ulcers, photosensitive rashes, psychotic illness, serositis with pleural and probably pericardial effusions and renal disease with nephrotic syndrome (Fig. 8.7). The high JVP might indicate early tamponade.
How would you manage this patient?
The next priority is to determine the extent and severity of the renal disease. Serum creatinine, eGFR, albumin, 24-h urine protein are essential. If there is an ‘active’ (p. 245) urine sediment, e.g. fragmented red cells and granular casts, indicating glomerulonephritis, renal biopsy is indicated.
Investigations
• FBC with reticulocyte count/Coombs’ (direct anti-globulin test) if positive: the anaemia is haemolytic
• U&Es (eGFR): renal impairment may be present
• Biochemistry: serum albumin will be low
• 24-h urine protein should be started
• Urine cytology for fragmented red cells and granular casts: a useful marker of glomerulonephritis
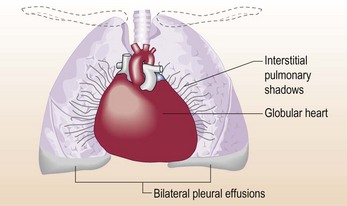
• CXR: to document pleural effusions and cardiomegaly (Fig. 8.8)
• Echocardiogram: to document pericardial effusion and possible valve lesions
• Blood cultures/urine cultures: to exclude sepsis, especially endocarditis, prior to corticosteroid and immunosuppressive therapy
• Full autoantibody screen: ANA, DNA, ENA, Rh factor, anti CCP, anti-cardiolipin antibodies, lupus anti-coagulant, ANCA
Other points
• Thrombosis prophylaxis: this patient is at high risk of deep vein thrombosis (DVT)/pulmonary embolus (PE). TED stockings and prophylactic low molecular weight heparin should be given.
• Is the anaemia haemolytic? If so, it should respond to corticosteroids.
• When the blood pressure has normalised as a result of treatment of the tamponade, start an ACE inhibitor. This is especially useful in proteinuric patients.
• If renal biopsy confirms proliferative glomerulonephritis: the treatment of choice is corticosteroid therapy and intermittent intravenous cyclophosphamide followed by azathioprine.
• This patient’s lipid profile might well be deranged, especially in the nephrotic syndrome. This will need to be assessed and managed actively. Measurement of serum lipids is performed and the patient started on a statin immediately if hypercholesterolaemia is present.
• Prophylaxis against corticosteroid-induced osteoporosis. A baseline dual energy X-ray absorptimetry (DXA) scan should be performed and calcium supplementation should be started.
Thrombosis and the anti-phospholipid syndrome
What is the differential diagnosis and your management?
Investigations
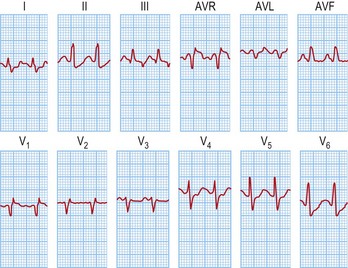
• An ECG: looking for the classic (but seldom seen) S1, Q3, T3 pattern of PE (Fig. 8.9)
• A CXR: but this is likely to be normal. However, it is useful to exclude other causes of pleuritic chest pain, including infective causes
• An ultrasound scan of the leg veins to document the extent of the left calf thrombosis
• A V/Q scan to show the extent of the pulmonary emboli is still useful if CT not available
• Plasma D-dimers: if undetectable the diagnosis of PE and DVT is excluded
• Multidetector CT with contrast: good specificity 96% and sensitivity 85% for medium-sized PEs
• Choose the imaging techniques according to local availability
Crystal arthritis
How would you manage this patient?
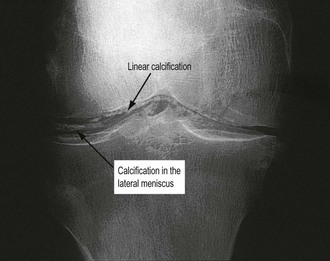
The X-ray showed chondrocalcinosis (Fig. 8.10) and patello-femoral and tibio-femoral osteoarthritis. The serum uric acid was elevated (520 µmol/L); she is taking a thiazide diuretic. The differential diagnosis thus includes gout or pseudo-gout, of which pseudo-gout is probably more likely in this clinical context. The uric acid level, although high, is usually > 600 µmol/L with gout.
Pseudo-gout
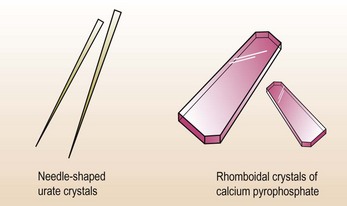
Calcium pyrophosphate is the most common crystal associated with pseudo-gout (Fig. 8.11). The crystals are diagnosed on synovial fluid analysis using polarised light microscopy. They are rhomboidal and positively birefringent and can be idiopathic or associated with osteoarthritis. A number of metabolic conditions are also associated with calcium pyrophosphate deposition; these include hypothyroidism, hyperparathyroidism, acromegaly, Wilson’s disease, haemochromatosis, hypophosphatasia and hypomagnesaemia.
Polymyalgia rheumatica/cranial arteritis
Acute back pain
Discuss your further investigations, diagnosis and management
The most urgent investigation is imaging of the lumbar spine and pelvis; magnetic resonance imaging (MRI; Fig. 8.12). The patient should be catheterised and analgesia given. This includes intramuscular non-steroidals such as IM diclofenac or opiate analgesics including morphine if needed. The patient should be referred immediately to a neurosurgeon or orthopaedic surgeon with an interest in acute spinal problems for urgent decompressive surgery with a laminectomy and discectomy. Any delay in diagnosis or decompression might lead to a permanent neurological deficit.

Severe back pain/osteoporosis
Discuss your differential diagnosis and management in this case
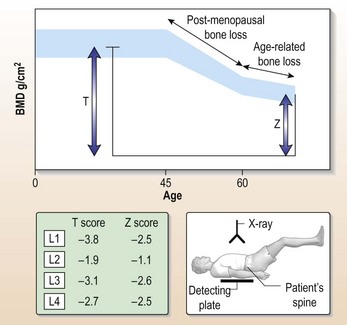
A DXA scan is performed to establish the degree of osteoporosis (Fig. 8.13). This gives an accurate index of bone mineral density in relation to the normal range for an age-, sex- and race-matched population. The World Health Organization definition of osteopenia is a T score of between –1.5 and 2.5. The definition of osteoporosis is a T score of greater than –2.5 standard deviations below the mean and established or severe osteoporosis is a T score of greater than –2.5 with an established fracture.
Osteomyelitis
A thoracic spine radiograph was normal. A chest X-ray showed no evidence of tuberculosis.
What is the differential diagnosis?
The most useful investigation is an MRI scan of the thoracic spine. This showed destruction of the vertebral body T4 with evidence of discitis T4/T5. A paravertebral abscess accompanied the bone destruction. These findings are typical of thoracic spine tuberculosis. There was no evidence of cord compression so a neurosurgical opinion was not required. Aspiration of the vertebral abscess was carried out to culture the tubercle bacillus and to obtain the sensitivities. She was commenced on isoniazid, pyrazinamide, rifampicin and ethanbutol, to be given for 9 months (reducing drugs when sensitivities known, p. 362). Other risk factors should always be considered, such as immunosuppression and HIV disease.
Septic arthritis
How would you investigate and manage this patient?
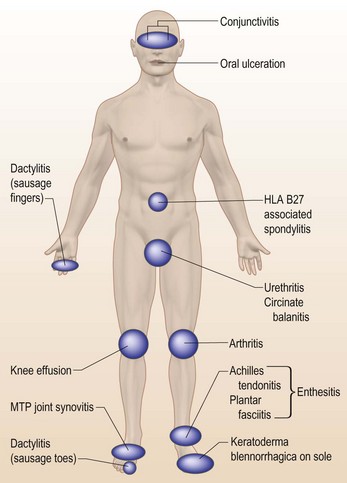
The most common diagnosis in a young man with a monoarthritis is a reactive arthritis associated either with diarrhoea or with urethritis, usually chlamydial in origin (Fig. 8.14). However, clinical questioning with this man has excluded any associated features that would point to reactive arthritis (a triad of urethritis, arthritis and conjunctivitis – Reiter’s disease)and septic arthritis should be considered as the most likely diagnosis, raising the possibility of HIV disease.
The joint should be X-rayed and a series of blood cultures performed following admission to MAU.
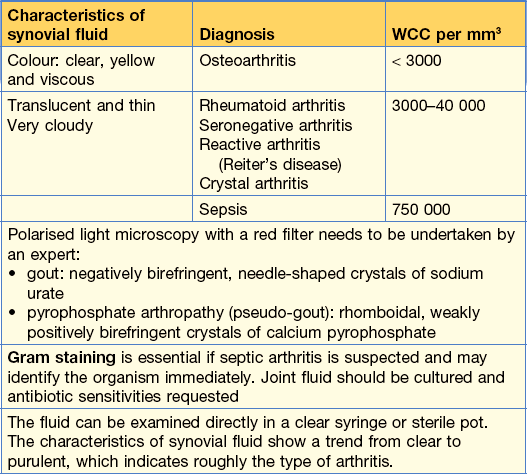
Information – knee aspiration
Progress.
In this man, a septic arthritis was confirmed on blood and synovial fluid culture (Table 8.2) due to Staph. aureus infection. He required 6 weeks of intravenous antibiotics, flucloxacillin plus oral fucidic acid. Arthroscopic drainage and washout of the joint was performed at 48 hours, which minimised joint damage.