127 Rheumatoid hands
Salient features
Examination
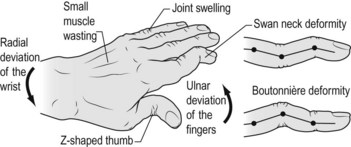
• Comment on deformities (Fig. 127.1) such as the following:
• Comment on the following signs:
• Test grip and pincer movements. Quickly test for abductor pollicis brevis and interossei, and pinprick sensation over index and little fingers. The median nerve may be involved if there is associated carpal tunnel syndrome.
• Examine the elbow for rheumatoid nodules.
• Ask the patient to perform simple tasks involving hand function, such as unbuttoning clothes or writing.
• Tell the examiner that you would like to examine other joints.
Questions
What is the significance of nodules in rheumatoid arthritis?
The presence of nodules indicates seropositive and more aggressive arthritis (Fig. 127.2).

Where are nodules found?
Flexor and extensor tendons of the hand, sacrum, Achilles tendon, sclera, lungs and myocardium.
What factors have been implicated in anaemia of chronic disease?
What precautions are necessary before upper gastrointestinal endoscopy or general anaesthesia?
It is prudent to take a cervical spine radiograph to rule out atlanto-axial subluxation.
Advanced-level questions
If the patient is known to experience gastric distress with non-steroidal anti-inflammatroy drugs, what precautions would you take while prescribing them?
What is Sjögren syndrome?
• The association of keratoconjunctivitis sicca (lack of lacrimal secretion) and xerostomia (dry mouth as a result of lack of salivary gland secretion) in association with a connective tissue disorder, usually rheumatoid arthritis. This syndrome may be associated with autoimmune thyroid disease, myasthenia gravis or autoimmune liver disease.
• Anti-Ro (SSA) and anti-SS-B antibodies may be seen in this syndrome.
• Treatment is symptomatic with artificial tears (hypomellose drops or 1% methylcellulose), artificial saliva and NSAIDs for the arthritis.
• The Schirmer filter paper test provides a crude measure of tear production. Filter paper is hooked over the lower eyelid and in normal people at least 15 mm is wet after 5 min, whereas in patients with keratoconjunctivitis sicca it is <5 mm.
What are the criteria for rheumatoid arthritis?
What are the factors leading to ulnar deviation of the hands?
In the normal grip, the fingers move to ulnar deviation; this is caused by:
• weakening of radial sides of the joint capsule and the radial insertion of the interossei ligaments
• the volar supports of the flexor tendon sheath are weakened by inflammation, allowing the tendon to bow in the direction of the ulna during gripping
• ulnar displacement of the extensor tendons in early deviation makes them slip if the dorsal metacarpophalangeal joint is taut, and this exacerbates the development of ulnar deviation by acting as a bowstring
• joint capsules of metacarpophalangeal joints are weaker on radial sides than on ulnar sides.






