Retropubic Vesicourethrolysis
The technique of retropubic or abdominal vesicourethrolysis has been described as a takedown of a retropubic repair that has resulted in urinary retention or significant voiding dysfunction. The goal of the operation is to free and mobilize the bladder and the proximal urethra. The procedure is performed as follows.
A large Foley catheter with a 30-mL balloon is placed inside the bladder. A transverse muscle–cutting incision, usually a Cherney incision (Fig. 35–1), is performed to facilitate exposure into the retropubic space. The bladder then is taken down sharply over the back of the symphysis pubis all the way down to the proximal urethra. It is best to make a high cystotomy to help in this dissection (Figs. 35–2 and 35–3). It is important to completely mobilize the bladder as well as the proximal urethra from the back of the symphysis. Very commonly, sutures or bone anchors from a previous suspension are encountered (Fig. 35–4). Dissection is extended laterally toward the pelvic sidewall and is taken down to the level of the arcus tendineus fasciae pelvis (white line) or the lower margin of the obturator internus fascia (Figs. 35–5 and 35–6). With the concern of rescarification in this area, it is at times beneficial to make a window in the peritoneum and bring in a piece of omentum to be placed between the back of the symphysis and the proximal urethra (Fig. 35–7). Usually resuspension is not necessary in these patients. If a high cystocele is noted following a paravaginal defect, a retropubic paravaginal repair is performed simultaneously.
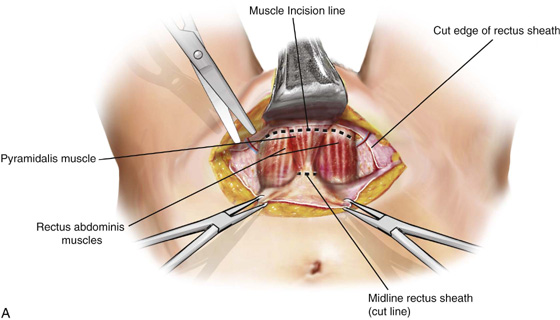
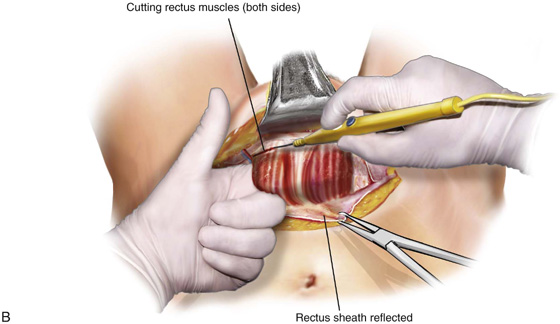
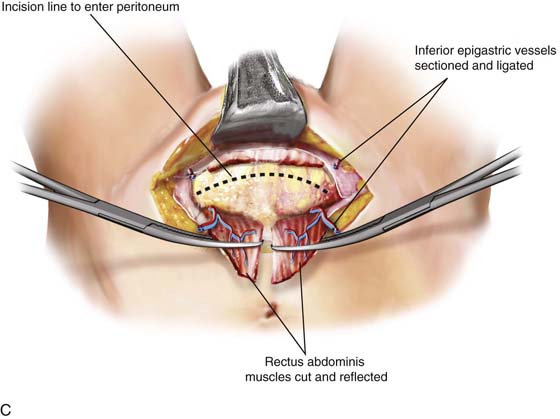
FIGURE 35–1 Technique for a Cherney muscle-cutting incision. A. A finger is taken around the entire belly of the rectus muscle. The finger should be behind the rectus muscle and in front of the peritoneum. The insertion of the muscle is then taken off the back of the symphysis by means of electrocautery. B. The muscle has been completely detached from its insertion. C. Easy access to the retropubic space is apparent once both rectus muscles have been cut.

FIGURE 35–2 Demonstrates the technique for a high extraperitoneal cystotomy, which is commonly performed during a retropubic vesicourethrolysis. A large Foley balloon has been placed in the bladder. The balloon is mobilized into the dome of the bladder. With an electrocautery pencil, the wall of the bladder is cut, creating the cystotomy.
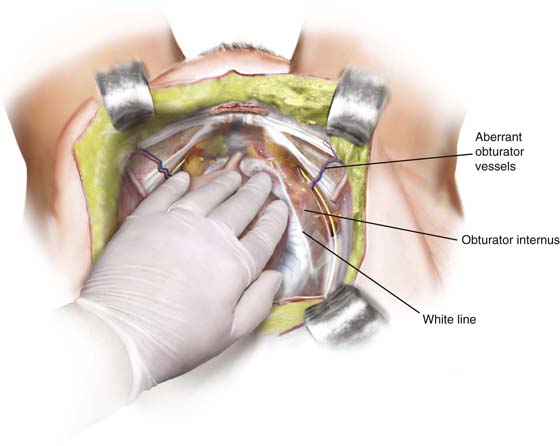
FIGURE 35–3 The technique of retropubic vesicourethrolysis involves sharp dissection, where the tissue is cut away from the back of the pubic bone.
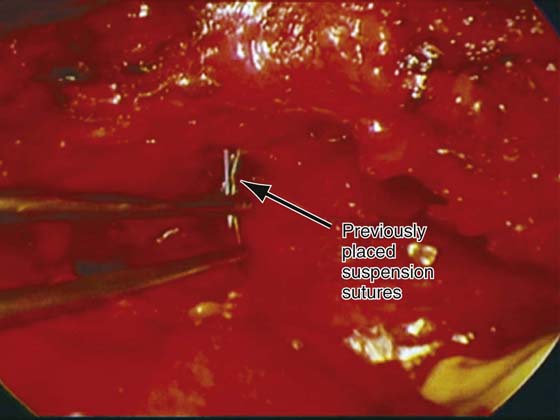
FIGURE 35–4 Previously placed suspension sutures are encountered and commonly are taken down during a retropubic vesicourethrolysis.
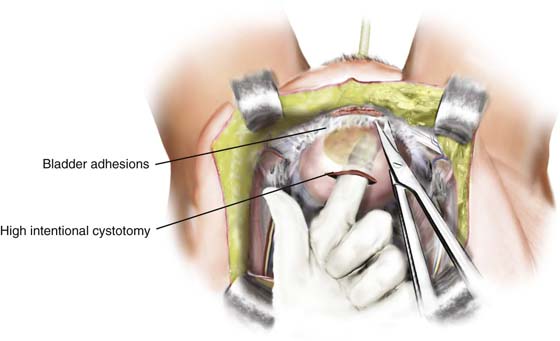
FIGURE 35–5 Retropubic vesicourethrolysis. A high extraperitoneal cystotomy has been made to facilitate sharp dissection of the bladder of the back of the symphysis pubis.
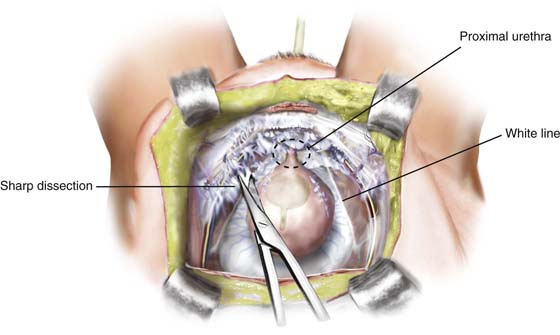
FIGURE 35–6 Sharp dissection is continued down in the midline until the proximal one third of the urethra has been mobilized off the symphysis. The dissection is extended laterally down to the level of the paravaginal attachment at the arcus tendineus fasciae pelvis (white line).
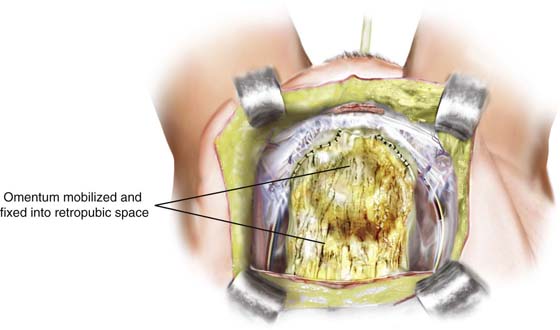
FIGURE 35–7 To prevent rescarification in this area, a piece of omentum can be brought through a window in the peritoneum. The omentum then is sutured at the midline to the lower aspect of the symphysis and laterally to the obturator fascia with numerous delayed-absorbable sutures.






