213 Retinal detachment
Salient features
Advanced-level questions
What are the types of retinal detachment?
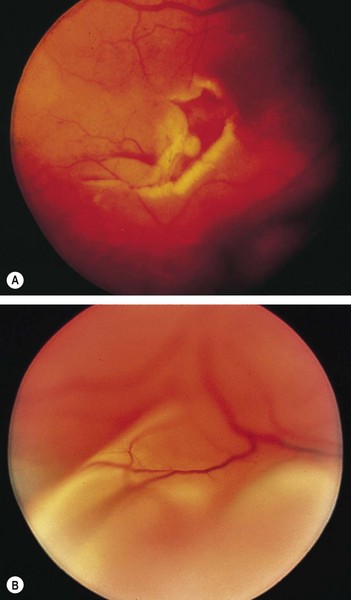
Rhegmatogenous retinal detachment. This is defined as the presence of a hole or break in the retina that allows fluid from the vitreous capacity to enter the subretinal space. It usually occurs spontaneously in those who have a predisposition to it following trauma to the eye or after intraocular surgery. Most of these patients develop symptoms. A break in the peripheral retina is associated with a sudden burst of flashing lights or sparks, which may be followed by small floaters or spots in the field of vision. When the retina detaches, the patient perceives a dark curtain progressing across the visual field, and when the fovea detaches central vision is abruptly diminished. It is treated surgically with a scleral buckling procedure.
Traction retinal detachment. This occurs when the intact retina is forcibly elevated by contracting membranes on the surface of the retina or by vitreous traction on areas of retinal neovascularization. Causes include diabetes, intraocular foreign body, perforating eye injuries and loss of vitreous humour following cataract surgery. These retinal detachments are difficult to treat and pars plana vitrectomy is the only option.
Secondary retinal detachments. This occurs secondary to systemic disorders including hypertension, toxaemia of pregnancy, chronic glomerulonephritis, retinal venous occlusive disease and retinal vasculitis. Treatment is directed towards the underlying cause as these detachments are not amenable to scleral buckling surgery.
What surgical procedures are available for retinal detachment?
• Scleral buckling is an extraocular approach that indents the eye wall to restore contact with the detached retina. All retinal breaks are localized and adhesions between the choroid and retina are performed around the break with diathermy or a cryoprobe. After draining the subretinal fluid, the detached portion of the retina is indented towards the vitreous cavity by a scleral implant or explant. This pushs the retina towards the vitreous humour, causing closure of the retinal break (by the buckled sclera and choroid) and release of traction on the vitreous humour.
• Pars plena vitrectomy is an intraocular approach that relieves traction by removing the vitreous humour attached to the retinal breaks, permitting reapproximation to the retinal pigment epithelium, where the breaks are permanently closed with retinopexy.
• Pneumatic retinopexy closes retinal breaks using a small bubble of pure sulfur hexafluoride or perfluoropropane injected intravitreally; this allows the retinal pigment epithelium pump to reattach the retina. Gradual elution of gas from the eye coupled with permanent closure of the break by retinopexy leaves the retina reattached. The initial studies utilizing this procedure involved treatment of primary detachments with small breaks that were restricted to the superior two-thirds of the fundus.





