Chapter 34 Respiratory diseases
Sinuses
As discussed in Chapter 15 ‘Methods of administration’ (p. 120), the thin, highly vascular lining of the sinuses makes it easy to reach with soluble orthodox medication (in the form of sprays) and vapourized aromatic oils. This, combined with their fat solubility, ensures rapid absorption into the body and also the brain.
Allergies
An allergic reaction is the body’s response to an antigen (see Chapter 30 ‘Inflammation and the immune system’, p. 225). This reaction can range from allergic rhinitis, hay fever and urticaria to drug hypersensitivities. The respiratory system plays a significant role in allowing allergens to enter the body.
The initial allergic reaction occurs in the following way:
A second exposure to the antigen activates a much greater response from the immune system, as the mast cells break open releasing histamines that react on mucosal membranes, smooth muscle, skin or other organs. The mast cells are concentrated at sites that are likely to incur most injury, e.g. mouth, nose, feet, blood vessels, skin, lungs and gut mucosa. This can create a problem if the mast cell activity gets out of hand and tissues from a variety of areas – from skin and joints to internal organs – are affected.
Allergic Rhinitis and Hay Fever
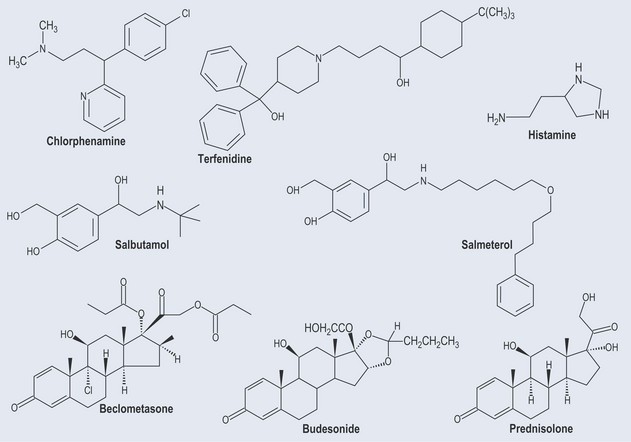
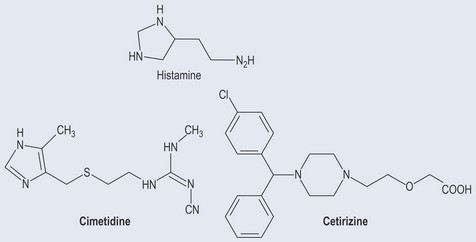
• Antihistamines
Histamine
Respiratory Diseases
Asthma
• Beta-2 Adrenoceptor Agonists
Beta-2 adrenoceptor agonists (see Chapter 31 ‘The nervous system’, p. 244) are used; these:
Usually, different types of medication are given: