Radical Vulvectomy With Tunnel Groin Dissection
A retrograde “tunnel” en bloc groin dissection commenced at the labial-crural fold is described (Fig. 72–1A). The procedure spares conventional inguinal incisions such as the “Texas Longhorn” incision (Fig. 72–1B) or the separate less radical groin incisions (Fig. 72–1C). Advantages include preservation of the groin skin layer, avoidance of incisional groin infection, and lymphedema of the legs. In our experience, operating time and hospitalization are markedly shortened.
This technique approaches easily the vulvar sentinel nodes because the fossa ovalis and the junctions of the femoral and greater saphenous veins are in close proximity to the labial-crural fold. The skin flap is raised from the labial-crural fold (Fig. 72–2) and is developed by sharp and blunt dissection (Fig. 72–3) until the underlying area of the fossa ovalis is reached. Sentinel groin nodes can then be removed from the fossa ovalis with adequate exposure (Fig. 72–4).
A classic en bloc specimen radical vulvectomy with bilateral groin dissection is outlined in Figure 72–5. Covering gauze is stapled over the tumor. The radical vulvectomy incision is started anteriorly. The skin flap is raised (Fig. 72–6) and developed by sharp and blunt dissection (Fig. 72–7). The surgical field is exposed by Deaver retractors. Vessels are transected by an electrosurgical device (Fig. 72–8). The fat pad is dissected from lateral to medial over the femoral triangle (Fig. 72–9).
Photographs show the exposure of the surgical field. The groin skin is exposed for assessment of thickness of the skin flap, although a groin incision is not made (Fig. 72–10). The specimen is rapidly developed from the area above the pubis and inguinal ligaments (Fig. 72–11). Dissection of the nodal fat pad over the femoral triangle is more delicate and is performed in traditional fashion with excellent exposure (Fig. 72–12). Tunnel groin dissection allows adequate surgical resection (Fig. 72–13).
The surgical field is tightly reapproximated (Fig. 72–14). Only one wound suction drain is inserted. We choose to use postoperative pressure dressings secured by stay sutures placed through the groin and anchored to the underlying fascia.
Because the pressure dressings are not covering an underlying wound, they do not get soiled and can remain in place for 1 week; they usually are removed in the office (Fig. 72–15). Postoperatively, the closed wound is covered with an antibiotic ointment.
Tunnel groin dissection is used mainly in T1 and T2 lesions. The operation avoids groin incision complications.
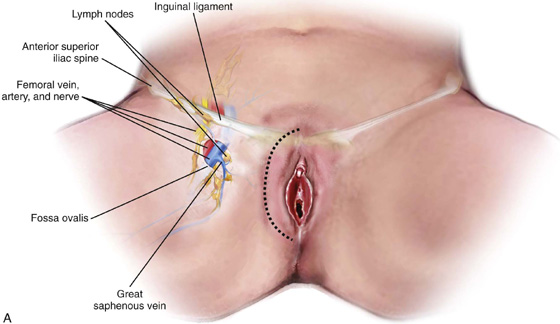
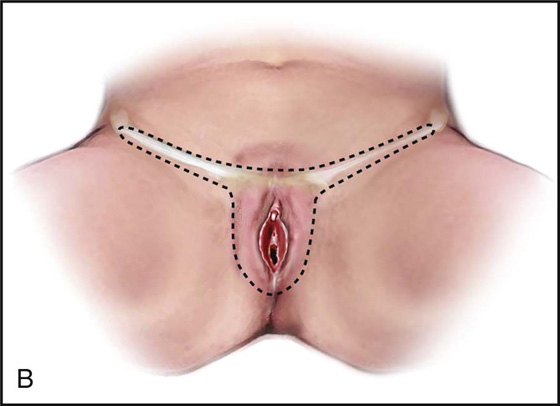
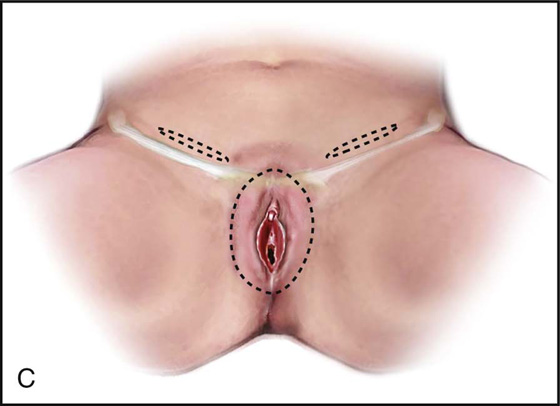
FIGURE 72–1 Different incisional approaches to radical vulvectomy with groin dissection are outlined. A. The lateral incision along the labial-crural fold used for the radical vulvectomy is also used to develop the skin flap over the femoral triangle with extension of the dissection above the inguinal ligaments and pubis. The proximity of the fossa ovalis and its vascular structures to the labial-crural fold is emphasized. B. The single Texas Longhorn incision, which is illustrated, is a more skin-sparing technique than the historical butterfly incision. C. A conservative three-incision technique is presently the preferred approach to groin dissection (see Fig. 72–1B); however, it does not allow en bloc dissection.
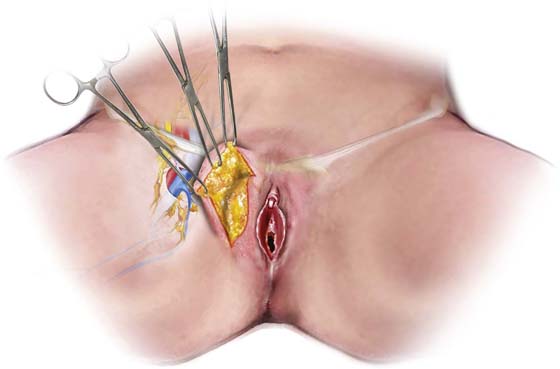
FIGURE 72–2 The skin flap for groin node dissection is raised.

FIGURE 72–3 Much flap development is performed by finger dissection.
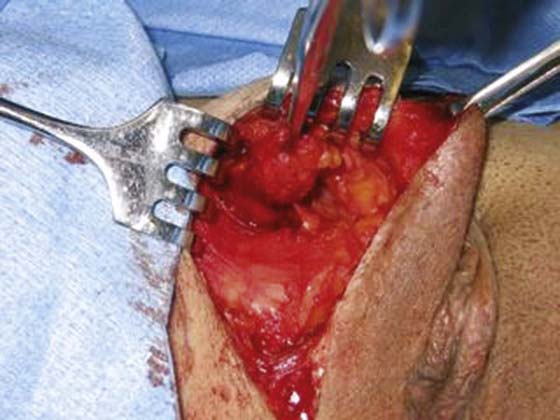
FIGURE 72–4 The fossa ovalis is exposed and lymph nodes are removed in a patient who underwent biopsy of the sentinel nodes only.
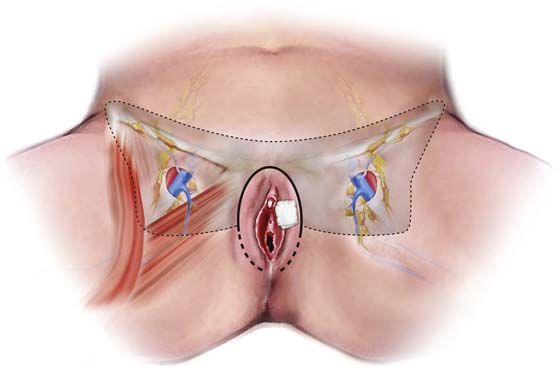
FIGURE 72–5 The extent of the bilateral groin dissection is outlined in the shaded area. The vulvar lesion has been covered with gauze. Initially, only the upper part of the radical vulvectomy incision is used to develop the groin skin flaps.
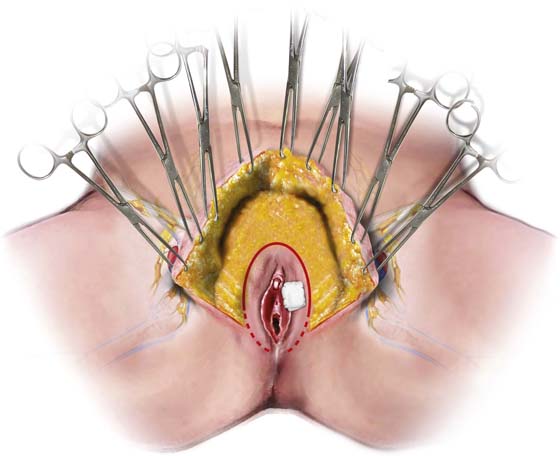
FIGURE 72–6 The skin flaps are raised from the upper groin dissection.
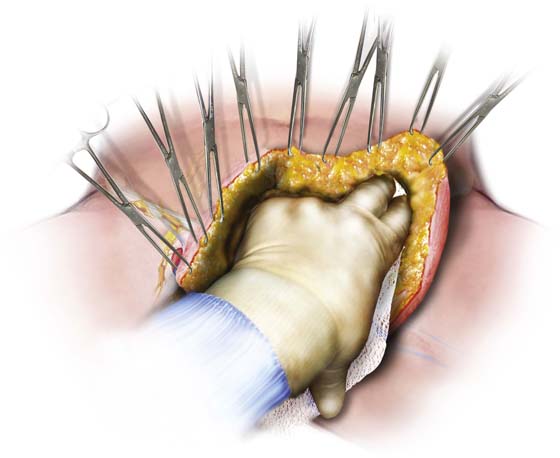
FIGURE 72–7 Much of the skin flap is performed by full dissection. Use of dry gauze facilitates the dissection of fatty tissue.
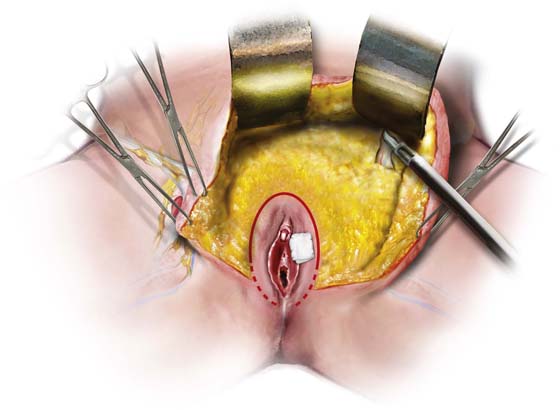
FIGURE 72–8 Both flaps are raised in continuity. Vascular structures are transected and cauterized with an electrosurgical device.
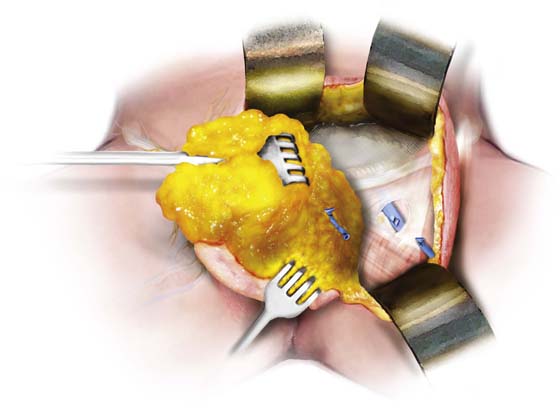
FIGURE 72–9 The fat pad is dissected from lateral to medial over the tunnel triangle. The greater saphenous vein is transected at the fossa ovalis.

FIGURE 72–10 Illustration of a case before surgery. Gauze is stapled over the tumor.
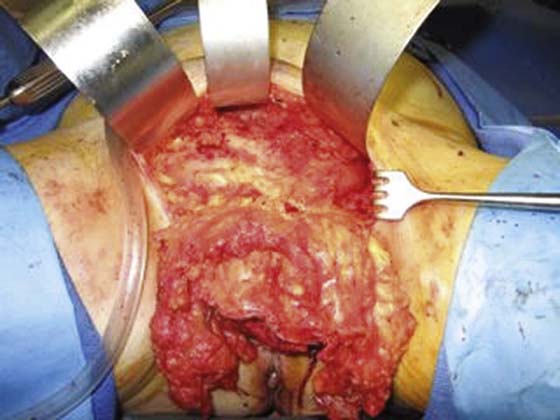
FIGURE 72–11 En bloc development of the surgical specimen over the lower abdominal fascia.
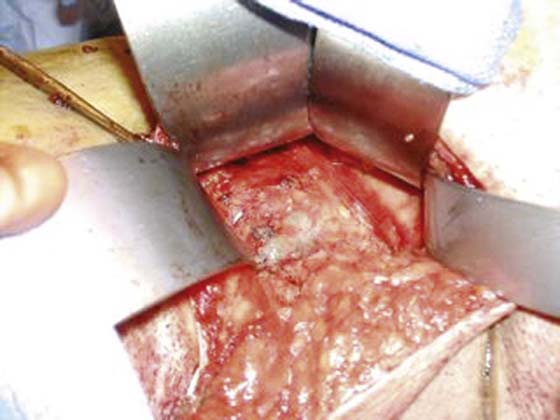
FIGURE 72–12 The femoral triangle is exposed with the femoral vein after transection of the greater saphenous vein.

FIGURE 72–13 Radical vulvectomy specimen.

FIGURE 72–14 The reapproximated wound bed. One suction catheter drains the surgical beds of both groins.

FIGURE 72–15 Pressure dressings are tied with stay sutures over both groins. Wide mattress sutures are anchored to the underlying fascia. The incision is covered with an antibiotic ointment.






