Racially pigmented skin
Common dermatoses may show variable manifestations in different races due to differences in pigmentation, hair or the response of skin to external stimuli. In addition, some conditions have a distinct racial predisposition. The response of darkly pigmented skin to injury and to certain therapeutic modalities needs to be taken into account when planning a programme of management.





Racial differences in normal skin
The most obvious difference is in pigmentation (p. 74), but hair forms and colour also vary. Mongoloid hair is straight and has the largest diameter; black African hair is short, spiralled, drier and more brittle than that of other races; and caucasoid hair may be wavy, straight or helical. Hair colour is predominantly black in mongoloids and Africans, and black, blond or red in caucasoids. Body hair is most profuse in caucasoids. The black African stratum corneum differs from that of the caucasoid by showing greater intercellular adhesion and a higher lipid content.
Diseases that show racially dependent variations
In pigmented skin, eruptions that appear red or brown in white caucasoid skin may be black, grey or purple, and pigmentation can mask an erythematous reaction. Inflammation in pigmented skin often provokes a hyperpigmentary (Figs 1 and 2) or hypopigmentary (Table 1) reaction. Follicular, papular and annular patterns are more common in pigmented skin than in caucasoid. In addition, some skin disorders show an inter-racial variation in prevalence (Table 2).


| Division | Disorder |
|---|---|
| Infections | Leprosy, onchocerciasis, pinta, pityriasis versicolor |
| Papulosquamous disorders | Pityriasis rosea, pityriasis alba, psoriasis (occasionally), seborrhoeic dermatitis |
| Physical and chemical agents | Burns, cryotherapy, hydroquinone, topical potent steroids |
| Post-inflammatory | Discoid lupus erythematosus, systemic sclerosis, sarcoidosis |
| Other | Albinism, vitiligo |
Diseases with a distinct racial or ethnic predisposition
Hair disorders
Racially dependent hair conditions are most common in black Africans and include the following:
 Folliculitis keloidalis describes discrete follicular papules, often keloids, at the back of the neck in African males (Fig. 3). Intralesional steroids may help.
Folliculitis keloidalis describes discrete follicular papules, often keloids, at the back of the neck in African males (Fig. 3). Intralesional steroids may help.
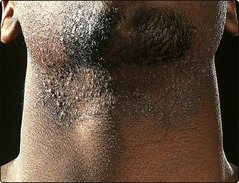
 Pseudofolliculitis barbae is a common disorder in black African men and is characterized by inflammatory papules and pustules in the beard area. It is thought to result from hairs growing back into the skin (Fig. 4). Treatment is difficult but includes attention to shaving technique and the topical use of antibiotics and steroids.
Pseudofolliculitis barbae is a common disorder in black African men and is characterized by inflammatory papules and pustules in the beard area. It is thought to result from hairs growing back into the skin (Fig. 4). Treatment is difficult but includes attention to shaving technique and the topical use of antibiotics and steroids.
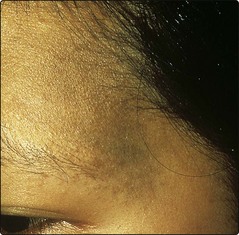
 Traction alopecia is mainly seen in black Africans because of the practice of plaiting or tightly braiding the hair (Fig. 5). Hairs are loosened from their follicles. The temples are often affected.
Traction alopecia is mainly seen in black Africans because of the practice of plaiting or tightly braiding the hair (Fig. 5). Hairs are loosened from their follicles. The temples are often affected.



Pigmentary changes





Other conditions
A racial preponderance is also seen with the following conditions:
 Sickle cell disease occurs in black Africans. The main cutaneous findings are painful oedema of the hands and feet, caused by infarction in the small bones, and leg ulceration.
Sickle cell disease occurs in black Africans. The main cutaneous findings are painful oedema of the hands and feet, caused by infarction in the small bones, and leg ulceration.










