38 Ptosis and Horner syndrome
Salient features
Examination
In the examination if you notice ptosis then you must answer the following questions:
• Is ptosis complete or incomplete?
• Is it unilateral or bilateral?
• Is the pupil constricted (Horner syndrome) or dilated (third nerve palsy)?
• Are extraocular movements involved (third nerve palsy or myasthenia gravis)?
• Is the eyeball sunken or not (enophthalmos)?
• Is the light reflex intact (intact light reflex in Horner syndrome)?
If the patient has Horner syndrome, then quickly proceed as follows:
These should help in making a diagnosis of syringomyelia or Pancoast’s tumour.
Questions
What are the features of Horner syndrome?
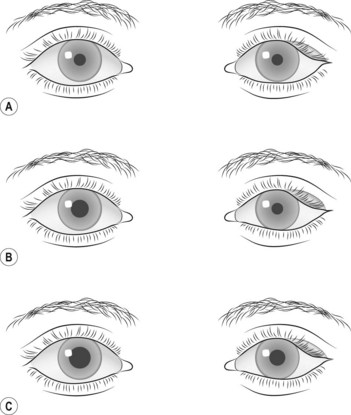
• miosis (resulting from paralysis of the dilator of the pupil) (Fig. 38.1)
• partial ptosis or pseudo-ptosis (caused by paralysis of the upper tarsal muscle)
• enophthalmos (caused by paralysis of the muscle of Müller)
• often, slight elevation of the lower lid (because of paralysis of lower tarsal muscles).
What additional feature would you see in congenital Horner syndrome?
There would be heterochromia of the iris: the iris remains grey–blue.
Advanced-level questions
How would you differentiate whether the lesion is above the superior ganglion (peripheral) or below the superior cervical ganglion (central)?
| Test | Above | Below |
|---|---|---|
| Sweating | Such lesions may not affect sweating at all as the main outflow to the facial blood vessels is below the superior cervical ganglion | Such lesions affect sweating over the entire, head, neck and arm upper trunk Lesions in the lower neck affect sweating over the entire face |
| Cocaine 4% in both eyes | Dilates the normal pupil, no effect on the affected side | Dilates both pupils |
| Epinephrine (adrenaline, 1:1000) in both eyes | Dilates affected eye, no effect on normal side | No effect on both sides |






