49
Pseudofolliculitis barbae

Multiple follicular pink papules in the beard region. The lesions often resolve with hyperpigmentation.

Numerous scattered inflammatory papules where skin has been shaved. Leaving beard length long prevents the problem of pseudofolliculitis. The problem is often more severe on the neck.

Tiny hairs piercing the skin, each hair surrounded by an erythematous halo. This reaction is not infectious, rather a foreign body-type reaction to coarse or curved hair piercing the skin.
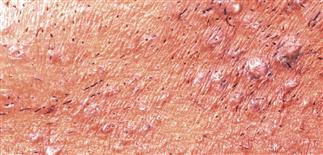
Papules in an area of skin where the hairs are shaved short. Some papules are pink and some are hyperpigmented. Close shaving predisposes.
DESCRIPTION
Pseudofolliculitis barbae is a papular and pustular, foreign body, inflammatory reaction that can affect any individual who has curly hair and regularly shaves closely.
HISTORY
• Significant problem in predisposed individuals who are required to shave closely. • Occurs commonly in African-American people; can be chronic and disfiguring. • Most severely affected sites are neck and beard areas. • Tends to be a chronic problem.
PHYSICAL FINDINGS
• Pseudofolliculitis barbae affects people with curly hair or with hair follicles oriented at oblique angle to skin surface. • A sharp, shaved, tapered hair reenters skin as it grows and induces a foreign body reaction, producing a microabscess. • Perifollicular red papules or pustules occur most commonly in beard area or any area where hair is shaved. • Lesions painful and/or pruritic. Scarring and hyperpigmentation may result. • Keloid formation is frequent problem.
TREATMENT
• Dislodge embedded hairs. A needle is inserted under hair loop, and the hair is firmly elevated. • A Buff Puff or toothbrush can be used to gently massage in a circular fashion and dislodge ingrown hair. • Discontinue shaving until inflammation under control. • Topical azelaic acid cream (Finacea) helps reduce hyperpigmentation and inflammation. • Topical antibiotic preparations (clindamycin, benzoyl peroxide 5% or 10%, erythromycin) reduce bacterial colonization. Culture, and if staph. aureus present, a short course of antistaphylococcal antibiotic appropriate for sensitivity may hasten resolution. • Intralesional triamcinolone acetonide 2.5 mg/mL used for persistent papules. Atrophy may result temporarily. • Once lesions resolve, shaving may be resumed. Avoid close shaves. • Shower before shaving and keep the beard hair in contact with warm water for at least 2 min. • Use thick-lathering shaving gels (Aveeno Therapeutic Shave Gel, Edge Gel for Tough Beards). • Bump Fighter razor (http://www.asrco.com) cuts the hair slightly above skin surface. • An electric razor can be used; avoid ‘closest’ shave setting. • Shave in the direction of hair growth. • A moisturizing lotion should be used after shaving. LactiCare-HC (1% or 2.5%) can be used intermittently. • Topical eflornithine hydrochloride 13.9% cream (Vaniqa) applied twice daily retards hair growth. Apply twice daily to affected skin. • Depilatories (Nair, Neet) are effective alternatives to shaving. Apply to skin for 3–10 min then wipe off. Irritation limits use to once or twice weekly. • If measures fail, discontinue shaving indefinitely. • Laser-assisted hair removal can provide a safe, effective means of treating recalcitrant cases.






