18 Prosthetic heart valves
Salient features
• Mitral valve prostheses can be recognized by their site, metallic first heart sound, normal second heart sound and metallic opening snap. Systolic murmurs are often also present and it is important to note that this does not indicate valve malfunction. Diastolic flow murmurs may be heard normally over the disc valves.
• Aortic valve prostheses may be recognized by their site, normal first heart sound and metallic second heart sound.
• Both mitral and aortic valves may be replaced and both the first and second heart sounds will be metallic. The presence of a systolic murmur does not indicate valve dysfunction. However, the presence of an early diastolic murmur indicates a malfunctioning aortic valve.
Note
• Comment on the midsternal vertical thoracotomy scar and state whether or not the metallic valve sounds are audible to the unaided ear (they are most often audible). Some mechanical valves cause so many clicks that it may not be possible to determine which valve has been replaced solely by auscultation. Porcine and cadaveric heterografts do not cause metallic clicking or plopping sounds.
Questions
What are the different kinds of valves?
Mechanical valves
• The Starr–Edwards valve is a caged ball device (Fig. 18.1C) and, because blood flows around the ball, there is a high incidence of haemolysis. This valve was introduced in 1960. The silastic ball is specially cured to prevent lipid accumulation (which can result in ball variance). The struts of the modern Starr-Edwards prosthesis are not covered with cloth.
• The Medtronic–Hall is a tilting disc valve (Fig. 18.1A) made of pyrolytic carbon. The disk tilts to an opening of 75 degrees for aortic prostheses and 70 degrees for mitral prostheses.
• The Bjork–Shiley pivoted single-tilting disc valve has laminar flow and hence a lower incidence of haemolysis. It was introduced in 1969. In the current model the entire ring and struts are machined from one piece (i.e. there are no welds). This is referred to as the ‘monostrut valve’.
• The St Jude valve is a double-tilting disc valve (bileaflet valve) (Fig. 18.1B). Other examples of bileaflet prostheses include Carbomedics and Duromedics valve.
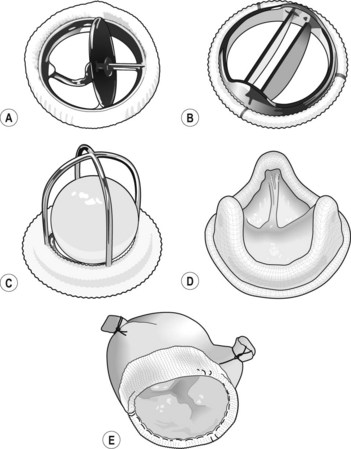
Xenografts
• Porcine valves (Fig. 18.1E; Carpentier–Edwards, Hancock Modified Orifice, C/E Duraflex, Medtronic Intact).
• Pericardial valves mounted on a frame (Mitroflow, Carpentier–Edwards pericardial, Ionescu–Shiley, Hancock). A design flaw predisposed the Ionescu–Shiley valve to sudden rupture of the cusps. Currently, the Baxter pericardial valve is being used but its long-term durability remains to be ascertained.
What are the complications of prosthetic valves?
• Valve dysfunction, including valve leakage, valve dehiscence and valve obstruction caused by thrombosis and clogging. Perivalvular leak is always abnormal. ‘Built-in’ transvalvular leakage should be <10 ml per beat. The loss of expected valve sounds is an important sign of mechanical valve thrombosis
• Bleeding (such as upper GI haemorrhage) caused by anticoagulants
• Haemolysis at valve, causing anaemia
• Endocarditis, which carries a mortality rate of up to 60%; patients should be urgently referred to a tertiary cardiothoracic centre (p. 80)
• Structural dysfunction: fracture, poppet escape, cuspal tear, calcification
• Non-structural dysfunction: paravalvular leak, suture/tissue entrapment, noise.
Notes
• All patients with prosthetic valve should have an echocardiogram performed 2 to 3 months after surgery to establish baseline values.
• When prosthetic valve dysfunction is suspected, transoesophageal echocardiogram is the procedure of choice but findings may be somewhat limited by acoustic shadowing and reverberations from prosthetic material.
Advanced-level questions
Is there any difference between the lifespan of a porcine mitral prosthesis and a porcine aortic prosthesis?
If a patient with atrial fibrillation requires a prosthetic mitral valve, which kind of valve would you prefer?
A mechanical valve, as these patients need warfarin treatment for atrial fibrillation.





