Chapter 14 Progressive Preoperative Pneumoperitoneum for Hernias with Loss of Abdominal Domain 
1 Clinical Anatomy
1 Features/Characteristics of the Defect
 Definition of Loss of Abdominal Domain
Definition of Loss of Abdominal Domain
 There is no consensus in the literature on the definition of loss of abdominal domain. Determination of this condition is subjective and typically refers to massive hernias with a significant amount of intestinal contents that have herniated through the abdominal wall into a hernia sac that forms a secondary abdominal cavity. On physical exam, the inability to reduce the herniated contents below the level of the fascia when the patient is lying supine should raise suspicion of the diagnosis. Although the surgeon can often make the assumption that a patient has loss of domain on physical exam, we utilize computed tomography (CT) to determine the true nature of the hernia.
There is no consensus in the literature on the definition of loss of abdominal domain. Determination of this condition is subjective and typically refers to massive hernias with a significant amount of intestinal contents that have herniated through the abdominal wall into a hernia sac that forms a secondary abdominal cavity. On physical exam, the inability to reduce the herniated contents below the level of the fascia when the patient is lying supine should raise suspicion of the diagnosis. Although the surgeon can often make the assumption that a patient has loss of domain on physical exam, we utilize computed tomography (CT) to determine the true nature of the hernia.2 Measuring Loss of Domain
 We define a loss of abdominal domain on CT scan as greater than 50% of the intestinal contents lying outside the native abdominal cavity in the hernia sac. This may be more accurately defined when the ratio of the volume of the hernia sac to the volume of the abdominal cavity is ≥0.5.
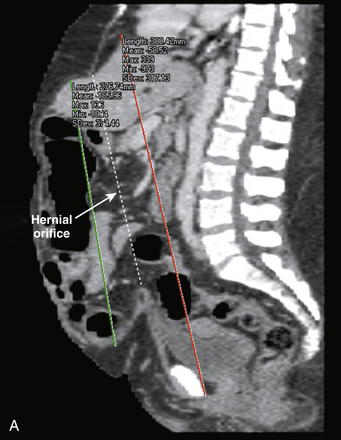
We define a loss of abdominal domain on CT scan as greater than 50% of the intestinal contents lying outside the native abdominal cavity in the hernia sac. This may be more accurately defined when the ratio of the volume of the hernia sac to the volume of the abdominal cavity is ≥0.5. A sagittal reconstruction of the CT scan is used to measure the length of the hernia sac from the top to the bottom of the sac. The length of the abdominal cavity is measured from the top of the diaphragm to the inferior aspect of the symphysis pubis (Fig. 14-1, A).
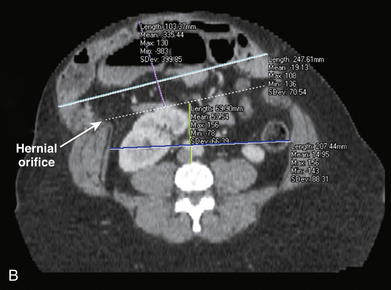
A sagittal reconstruction of the CT scan is used to measure the length of the hernia sac from the top to the bottom of the sac. The length of the abdominal cavity is measured from the top of the diaphragm to the inferior aspect of the symphysis pubis (Fig. 14-1, A). Axial reconstructions are used to measure the width of the hernia sac and abdominal cavity at their widest point. The height of the hernia sac is measured from an imaginary line drawn across the hernial orifice to the apex of the hernia sac at its tallest portion. The height of the abdominal cavity is measured from the anterior portion of the fourth lumbar space to an imaginary line drawn across the hernial orifice (see Fig. 14-1, B).
Axial reconstructions are used to measure the width of the hernia sac and abdominal cavity at their widest point. The height of the hernia sac is measured from an imaginary line drawn across the hernial orifice to the apex of the hernia sac at its tallest portion. The height of the abdominal cavity is measured from the anterior portion of the fourth lumbar space to an imaginary line drawn across the hernial orifice (see Fig. 14-1, B).
 Physiology of Hernias with Loss of Abdominal Domain
Physiology of Hernias with Loss of Abdominal Domain
 In patients with loss of abdominal domain, the bowels reside outside the abdominal cavity. As intraabdominal pressure decreases to approach atmospheric pressure, abdominal viscera become edematous and their vasculature becomes engorged. This makes simple hernia reduction nearly impossible. In addition, respiratory function is altered secondary to the loss of diaphragmatic support, and anterior spinal support fails, leading to lordosis.
In patients with loss of abdominal domain, the bowels reside outside the abdominal cavity. As intraabdominal pressure decreases to approach atmospheric pressure, abdominal viscera become edematous and their vasculature becomes engorged. This makes simple hernia reduction nearly impossible. In addition, respiratory function is altered secondary to the loss of diaphragmatic support, and anterior spinal support fails, leading to lordosis.4 Physiology of Progressive Preoperative Pneumoperitoneum
 The immediate reintroduction of viscera and abdominal reconstruction in patients with loss of domain can result in a significant increase in intraabdominal pressure, which can lead to abdominal compartment syndrome and its resultant ill effects. Progressive preoperative pneumoperitoneum (PPP) attenuates the adverse physiologic effects associated with ventral hernia repair in patients with a loss of abdominal domain.
The immediate reintroduction of viscera and abdominal reconstruction in patients with loss of domain can result in a significant increase in intraabdominal pressure, which can lead to abdominal compartment syndrome and its resultant ill effects. Progressive preoperative pneumoperitoneum (PPP) attenuates the adverse physiologic effects associated with ventral hernia repair in patients with a loss of abdominal domain.


2 Preoperative Considerations
1 Physical Examination
 The physical exam alone is often helpful in determining whether a patient has loss of domain. With the patient lying supine on the examination table, the surgeon should attempt to reduce the herniated contents below the fascia. If the hernia does not reduce because of the amount of herniated contents, the patient likely has loss of domain
The physical exam alone is often helpful in determining whether a patient has loss of domain. With the patient lying supine on the examination table, the surgeon should attempt to reduce the herniated contents below the fascia. If the hernia does not reduce because of the amount of herniated contents, the patient likely has loss of domain


2 Computed Axial Tomography





3 Planning Abdominal Wall Reconstruction
 Weight Loss
Weight Loss






3 Operative Steps
1 Stage I
 Placement of Percutaneous Vena Cava Filter
Placement of Percutaneous Vena Cava Filter




 Exploratory Laparoscopy with Placement of Percutaneous Catheter System
Exploratory Laparoscopy with Placement of Percutaneous Catheter System
 Exploratory laparoscopy allows for minimally invasive access to the abdominal cavity for direct visualization and placement of a percutaneously placed intraperitoneal catheter system for the pneumoperitoneum.
Exploratory laparoscopy allows for minimally invasive access to the abdominal cavity for direct visualization and placement of a percutaneously placed intraperitoneal catheter system for the pneumoperitoneum.
 A peritoneal dialysis catheter is placed under direct vision, using the Seldinger technique with a percutaneous, tear-away introducer sheath (Fig. 14-3).
A peritoneal dialysis catheter is placed under direct vision, using the Seldinger technique with a percutaneous, tear-away introducer sheath (Fig. 14-3).










2 Stage II
 Progressive Preoperative Pneumoperitoneum
Progressive Preoperative Pneumoperitoneum

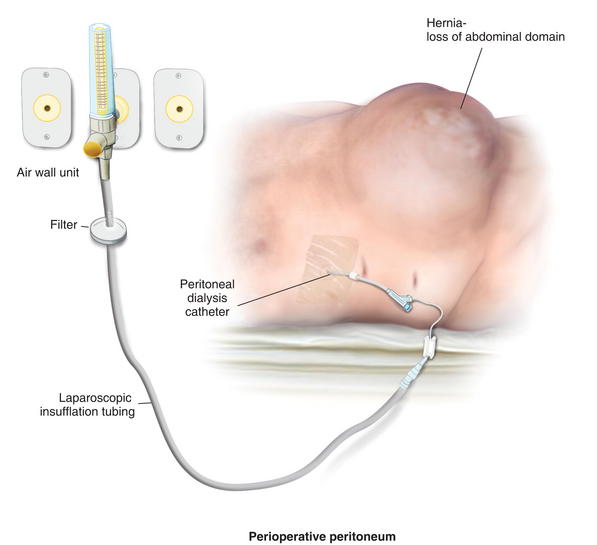
 Laparoscopic insufflation tubing is utilized to connect the air hose at the patient’s bedside to the peritoneal dialysis catheter (Fig. 14-5).
Laparoscopic insufflation tubing is utilized to connect the air hose at the patient’s bedside to the peritoneal dialysis catheter (Fig. 14-5).



 Repeat CT Scan to Determine Suitability for Stage III
Repeat CT Scan to Determine Suitability for Stage III
 After 7 days of daily PPP, a CT scan is performed to determine the suitability of the abdominal wall for repair.
After 7 days of daily PPP, a CT scan is performed to determine the suitability of the abdominal wall for repair.





3 Stage III
 Abdominal Wall Reconstruction
Abdominal Wall Reconstruction



 Rives-Stoppa with PCST
Rives-Stoppa with PCST
 After a complete lysis of adhesions a towel is placed intraperitoneally to protect the underlying viscera.
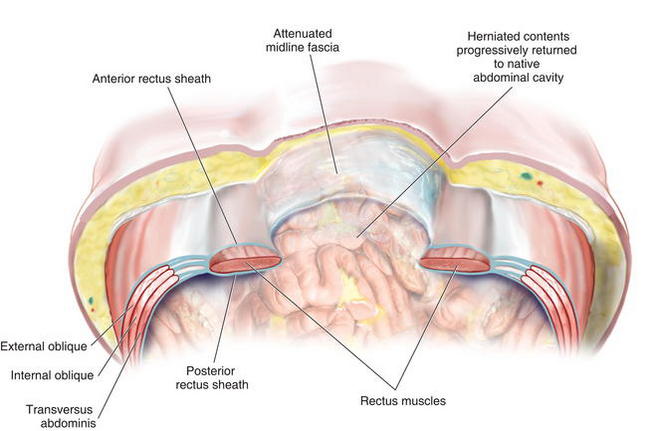
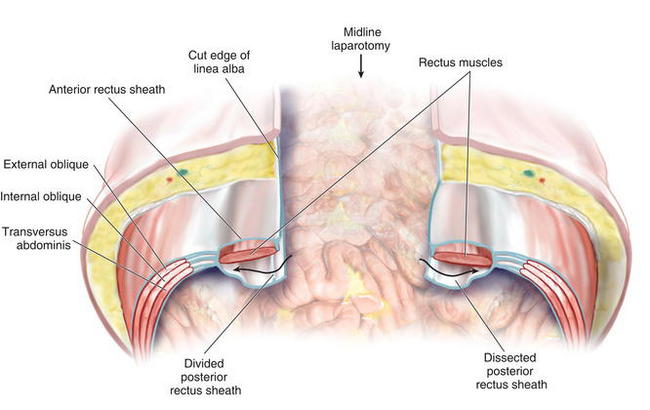
After a complete lysis of adhesions a towel is placed intraperitoneally to protect the underlying viscera. The posterior rectus sheath is divided vertically 1 cm or less from the edge of the linea alba and the division continues 5 cm cephalad to the hernia defect edge and 5 cm caudal to it (Fig. 14-10).
The posterior rectus sheath is divided vertically 1 cm or less from the edge of the linea alba and the division continues 5 cm cephalad to the hernia defect edge and 5 cm caudal to it (Fig. 14-10). The posterior rectus sheath is reflected posteriorly under tension and the rectus muscle is gently dissected off the ventral aspect of the sheath (Fig. 14-11).
The posterior rectus sheath is reflected posteriorly under tension and the rectus muscle is gently dissected off the ventral aspect of the sheath (Fig. 14-11).

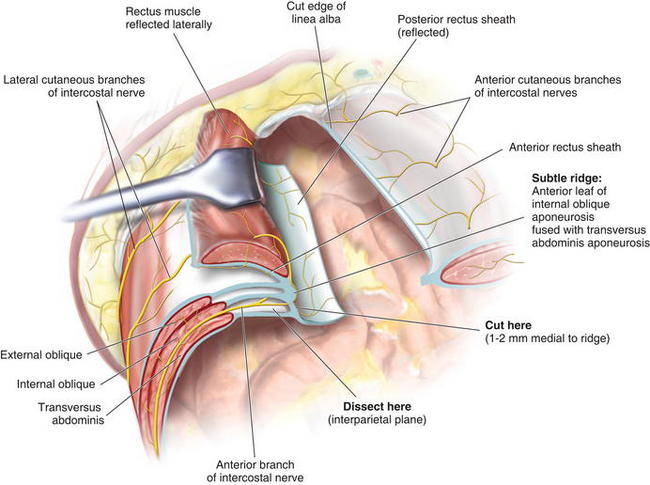
 For the PCST, the dissection is carried to the lateral most extent of the rectus sheath. With a Richardson retractor reflecting the rectus laterally at this lateral extent, a subtle ridge becomes evident. This ridge is formed by the rolled over anterior leaf of the internal oblique aponeurosis as it fuses with the transversus abdominis aponeurosis to form the posterior rectus sheath (Fig. 14-12).
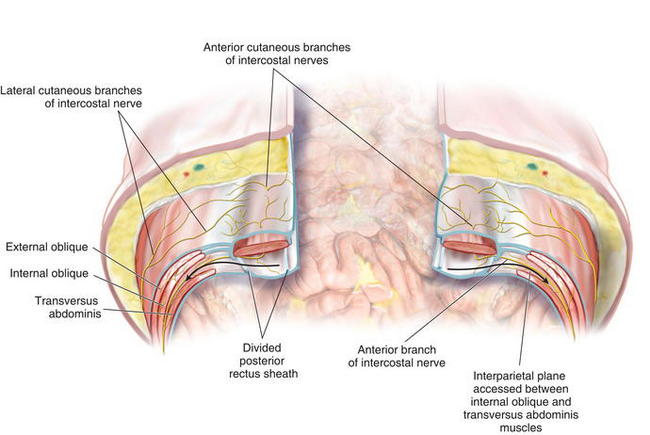
For the PCST, the dissection is carried to the lateral most extent of the rectus sheath. With a Richardson retractor reflecting the rectus laterally at this lateral extent, a subtle ridge becomes evident. This ridge is formed by the rolled over anterior leaf of the internal oblique aponeurosis as it fuses with the transversus abdominis aponeurosis to form the posterior rectus sheath (Fig. 14-12). By incising the fascia 1 to 2 mm medial to this ridge, the interparietal plane between internal oblique and transversus abdominis muscle is accessed, and the incision is continued for the entire length of the skin incision and beyond (Fig. 14-13).
By incising the fascia 1 to 2 mm medial to this ridge, the interparietal plane between internal oblique and transversus abdominis muscle is accessed, and the incision is continued for the entire length of the skin incision and beyond (Fig. 14-13).

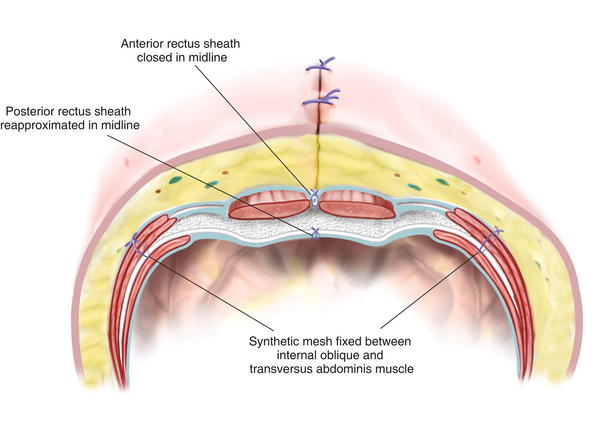
 The synthetic mesh is placed in the retromuscular space and fixated with full-thickness permanent transabdominal sutures utilizing the Reverdin needle (Fig. 14-14).
The synthetic mesh is placed in the retromuscular space and fixated with full-thickness permanent transabdominal sutures utilizing the Reverdin needle (Fig. 14-14).





4 Pearls/Pitfalls








Carbonell A., Cobb W.S., Chen S.M. Posterior components separation during retromuscular hernia repair. Hernia: the journal of hernias and abdominal wall surgery. 2008;12(4):359-362.
Mcadory R.S., Cobb W.S., Carbonell A.M. Progressive preoperative pneumoperitoneum for hernias with loss of domain. The American surgeon. 2009;75(6):504-508. discussion 508–509
Moreno. Chronic eventrations and large hernias. Preoperative treatment by progressive pneumoperitoneum-original procedure. Surgery. 1947;22:945-953.
Tanaka E.Y., Yoo J.H., Rodrigues A.J., Utiyama E.M., Birolini D., Rasslan S. A computerized tomography scan method for calculating the hernia sac and abdominal cavity volume in complex large incisional hernia with loss of domain. Hernia. 2010;14(1):63-69.
