45
Pityriasis lichenoides et varioliformis acuta

Lesions appear abruptly and are found primarily on the trunk and proximal extremities. There may be a few or more than one hundred discrete lesions.

Lesions may be asymmetrically distributed on the trunk.

Lesions may appear on the distal extremities and the palms and soles.
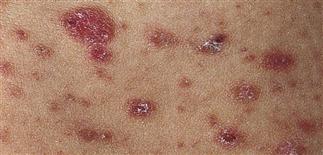
Red-brown, round to oval papules develop central necrosis, hemorrhage, and crust. Lesions are in different stages of development, as is seen in chickenpox.
DESCRIPTION
Rare papular eruption of unknown etiology and two variants. 1. Pityriasis lichenoides et varioliformis acuta (PLEVA) or Mucha–Habermann disease: acute form with rapid evolution of highly inflamed lesions. 2. Pityriasis lichenoides chronica: chronic form with slow evolution of mildly inflammatory lesions.
HISTORY
• Occurs at any age; most cases in first, second, and third decades. • Usually benign and self-limited but may wax and wane for years. • PLEVA presents with sudden onset of mildly itchy papules that rapidly evolve to vesicles and hemorrhagic crusts. The eruption clears in about 6 weeks. A severe form presents with ulceronecrotic lesions, high fever, and myalgias and other systemic symptoms. • The chronic form appears over several days; chronically inflamed lesions take 6–8 months to resolve.
PHYSICAL FINDINGS
• PLEVA: papules with adherent thin scale occur in crops. Round to oval, reddish-brown papules vary in size, become vesicular, and undergo hemorrhagic necrosis usually within 2–5 weeks, often leaving postinflammatory hyperpigmentation. Occurs most often on trunk and proximal extremities; face, scalp, palms, and soles sometimes involved. • Pityriasis lichenoides chronica: occurs primarily on trunk and consists of brownish-red papules with fine, mica-like, adherent scale.
TREATMENT
• Erythromycin (30–50 mg/kg q.d. for several weeks) or tetracycline is the most commonly used treatment. Response unpredictable. Group I–III topical steroids used b.i.d. provide some relief. Oral corticosteroids or dapsone may be effective for acute form. • Phototherapy with psoralen plus ultraviolet A and ultraviolet B, or ultraviolet B or narrowband ultraviolet B effective for chronic form. • Mentholated lotions (Sarna lotion) relieve itch.






