Pituitary function
The pituitary gland
Anterior pituitary hormones
 TSH (thyroid-stimulating hormone), acts specifically on the thyroid gland to elicit secretion of thyroid hormones.
TSH (thyroid-stimulating hormone), acts specifically on the thyroid gland to elicit secretion of thyroid hormones.




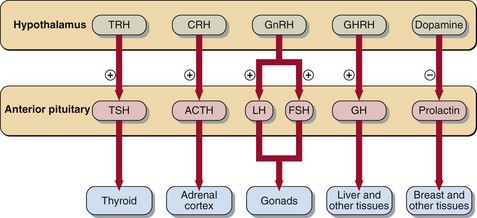
The hypothalamic factors that control anterior pituitary hormone secretion are shown in Figure 42.1.
Hyperprolactinaemia
 stress (venepuncture is sufficient to raise plasma prolactin in some patients)
stress (venepuncture is sufficient to raise plasma prolactin in some patients)
 drugs (e.g. oestrogens, phenothiazines, metoclopramide, α-methyl dopa)
drugs (e.g. oestrogens, phenothiazines, metoclopramide, α-methyl dopa)

 primary hypothyroidism (prolactin is stimulated by the raised TRH)
primary hypothyroidism (prolactin is stimulated by the raised TRH)

If these causes are excluded, the differential diagnosis is between:





Pituitary tumours
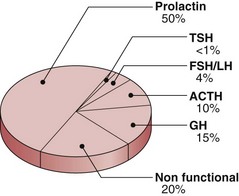
Pituitary tumours may be either functional (that is they secrete hormones) or non-functional. The incidence of different tumour types is shown in Figure 42.2. Local effects include headaches, papilloedema and visual field defects. There may be specific signs of hormone excess particularly in acromegaly, Cushing’s syndrome and prolactinoma. There may be signs of hypopituitarism in skin, hair and musculature.
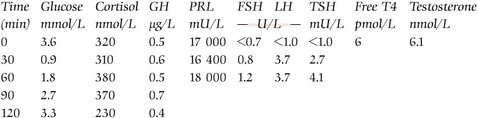
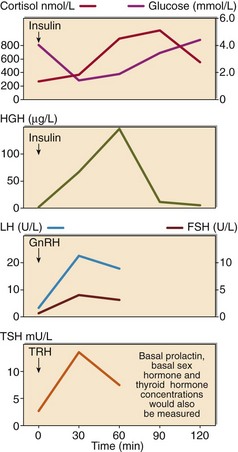
The impact of the tumour on pituitary function requires formal assessment by dynamic function tests. GH and ACTH-secreting cells are most vulnerable, and an insulin stress test (see p. 82) may suffice. However, comprehensive assessment of anterior pituitary reserve requires a combined anterior pituitary function test (Fig 42.3). TRH, GnRH and insulin are administered. All hormones are assessed at 0, 30 and 60 minutes, and GH additionally at 90 and 120 minutes. It is usual also to assess basal thyroid (thyroxine) and gonadal (testosterone or oestradiol) function.



Hypopituitarism
 Clinical note
Clinical noteCase history 32