123
Pilar cyst
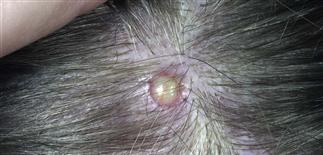
Pilar cysts are commonly found on the scalp, may interfere with hats or helmets, and are usually removed when symptomatic.

This large pilar cyst exerted pressure against the skin and has destroyed follicles.

Roughly 90% of cysts appear on the scalp, with the remaining 10% on the face, neck, back, and scrotum. Removal of scrotal pilar cysts can be accomplished by incision, similar to ones on scalp.

Pilar cysts rupture less frequently than epidermal cysts, as the pilar cyst has a thicker wall, making it firm and less mobile.
DESCRIPTION
Firm, subcutaneous, keratin-filled cyst originating from outer root sheath of hair follicle. Most commonly on scalp.
HISTORY
• Pilar cysts are less common than, but otherwise similar to, epidermal cysts. • Roughly 90% are on scalp; remaining 10% occur on face, neck, back, scrotum. • Epithelium of outer root sheath undergoes different form of keratinization than that of cutaneous epithelium. • Almost always develop after puberty. • Tendency to develop pilar cysts often has autosomal dominant inheritance. • Usually multiple in 70% of patients. • Persist indefinitely, grow slowly to a stable size unless they rupture. • Rupture less frequently than epidermal cysts, presumably because pilar cyst has thicker wall. Rupture usually results from external trauma. A brisk foreign body inflammatory reaction follows, can be quite painful, resembles a furuncle.
PHYSICAL FINDINGS
• Clinically indistinguishable from epidermal cysts, differing only in distribution. Both present as a firm, subcutaneous nodule, about 0.5 to 5.0 cm. • Pilar cysts have no central punctum, unlike epidermal cysts. When such a cyst is surgically dissected, the pilar cyst possesses a tough, white-gray wall more resistant to tearing than the wall of an epidermal cyst. Pilar cyst wall separates easily and cleanly from surrounding dermis. • If pilar cyst ruptures, area becomes inflamed, red, tender, boggy on palpation. • Large cysts may be cosmetically objectionable. Some cysts are so large and tender they may interfere with wearing hats, helmets. • Acute inflammation after rupture often misdiagnosed as infection. Antibiotics of little value in such cases. • Incision and drainage under local anesthesia improve comfort and limit scarring. Elective excision before rupture prevents this complication.
TREATMENT
• Easily removed with excision under local anesthesia. An incision is made over the cyst, exposing the glossy white external surface. Cyst wall is freed easily from surrounding connective tissue by blunt dissection. • At this stage, smaller cysts may be expressed intact up through the incision by steady, firm pressure on each side of incision. • Larger cysts, which cannot be expressed in this manner, should be incised and their contents removed by curettage. Incised cyst wall is clamped and, through a combination of gentle traction and pressure on each side of the incision, the now smaller, partially emptied cyst is delivered through the incision. If sutures are needed, they are placed and removed in 7–10 days.






