110 Pickwickian syndrome
Salient features
History
Examination
• Obese patient who is plethoric and cyanosed
• Maxillary or mandibular hypoplasia:
• Look for signs of pulmonary hypertension and right heart failure
• Tell the examiner that you would like to measure the neck circumference
Remember: Nearly 50% of patients with sleep apnoea syndrome are not obese.
Advanced-level questions
What is the cause of cyanosis in such a patient?
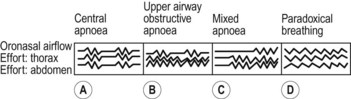
A mixture of obstructive apnoea and sleep-induced hypoventilation (Fig. 110.1). The blood gas picture is hypoxia and carbon dioxide retention.
Where is the obstruction?
It is caused by the apposition of the tongue and the palate of the posterior pharyngeal wall.
How would you treat such a patient?
• Avoidance of smoking and alcohol
• Continuous nasal positive airway pressure (CPAP) delivered by a nasal mask (Lancet 1999;353:2100–5). CPAP is recommended even if the apnoea–hypopnoea index is in the mild range (5 to 15), although evidence for the efficacy of CPAP is strong for patients with an apnoea–hypopnoea index >15. CPAP acts like a pneumatic splint (resulting in patency of the upper airway during inspiration and expiration). The resultant reductions in gas-exchange perturbations, respiratory effort, abrupt arousals and BP surges all probably ameliorate symptoms
• Surgery. Tracheostomy, uvulopalatopharyngoplasty, linguoplasty, mandibular advancement, plastic remodelling of the uvula (laser-assisted or radiofrequency ablation), tonsillectomy, reconstruction of maxillae
• Drugs: serotonin, receptor blockade, acetazolamide, methylxanthines, weight loss medications
• Atrial overdrive pacing may benefit selected patients (the vagal tone that accompanies bradycardia also causes the sleep apnoea, so prevention of the enhanced vagal tone prevents the apnoea) (N Engl J Med 2002;346:404–12).






