Phosphate and magnesium
Phosphate
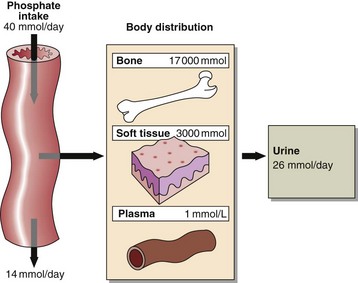
Phosphate is abundant in the body and is an important intracellular and extracellular anion. Much of the phosphate inside cells is covalently attached to lipids and proteins. Phosphorylation and dephosphorylation of enzymes are important mechanisms in the regulation of metabolic activity. Most of the body’s phosphate is in bone (Fig 37.1). Phosphate changes accompany calcium deposition or resorption of bone. Control of ECF phosphate concentration is achieved by the kidney, where tubular reabsorption is reduced by PTH. The phosphate that is not reabsorbed in the renal tubule acts as an important urinary buffer.
Hyperphosphataemia





Hypophosphataemia








Magnesium homeostasis
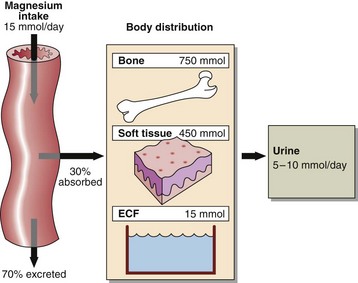
Since magnesium is an integral part of chlorophyll, green vegetables are an important dietary source, as are cereals and animal meats. An average dietary intake is around 15 mmol per day which generally meets the recommended dietary intake. Children and pregnant or lactating women have higher requirements. About 30% of the dietary magnesium is absorbed from the small intestine and widely distributed to all metabolically active tissue (Fig 37.2).
Magnesium deficiency
 dietary insufficiency accompanied by intestinal malabsorption, severe vomiting, diarrhoea or other causes of intestinal loss
dietary insufficiency accompanied by intestinal malabsorption, severe vomiting, diarrhoea or other causes of intestinal loss
 osmotic diuresis such as occurs in diabetes mellitus
osmotic diuresis such as occurs in diabetes mellitus
 prolonged use of diuretic therapy especially when dietary intake has been marginal
prolonged use of diuretic therapy especially when dietary intake has been marginal

 cytotoxic drug therapy such as cisplatin, which impairs renal tubular reabsorption of magnesium
cytotoxic drug therapy such as cisplatin, which impairs renal tubular reabsorption of magnesium

 Clinical note
Clinical note





