[level-membership-for-obstetrics-gynecology-category]
Chapter 249 Pessary Fitting
CPT CODE(S)
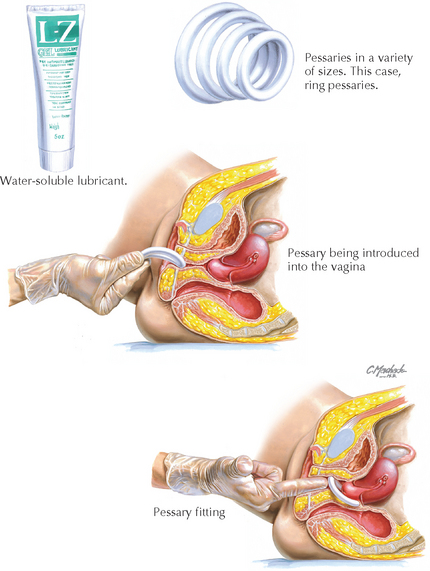
Indications for Common Pessaries
Malposition: Lever type (Hodge)
Uterine: Gellhorn, ring, doughnut, cube
Vaginal: Doughnut, cube, ball (Gehrung)
Cystocele/Rectocele: Gehrung, Schatz
Incompetent cervix: Lever, ring
Incontinence: Doughnut, lever, ring
Drug delivery: Specialized ring (17β-estradiol, medroxyprogesterone, prostaglandin E2)
Cundiff GW, Amundsen CL, Bent AE, et al. The PESSRI study: symptom relief outcomes of a randomized crossover trial of the ring and Gellhorn pessaries. Am J Obstet Gynecol. 2007;196:405.e1.
Clemons JL, Aguilar VC, Tillinghast TA, et al. Risk factors associated with an unsuccessful pessary fitting trial in women with pelvic organ prolapse. Am J Obstet Gynecol. 2004;190:345.
Mutone MF, Terry C, Hale D, Benson JT. Factors which influence the short-term success of pessary management of pelvic organ prolapse. Am J Obstet Gynecol. 2005;193:89.
Wu V, Farrell SA, Baskett TF, Flowerdew G. A simplified protocol for pessary management. Obstet Gynecol. 1997;90:990.
Adams E, Thomson A, Maher C, Hagen S. Mechanical devices for pelvic organ prolapse in women. Cochrane Database Syst Rev. 2, 2004. CD004010
American College of Obstetricians and Gynecologists. Pelvic organ prolapse. ACOG Practice Bulletin 79. Obstet Gynecol. 2007;109:461.
Anders K. Devices for continence and prolapse. BJOG. 2004;111:61.
Clemons JL, Aguilar VC, Tillinghast TA, et al. Patient satisfaction and changes in prolapse and urinary symptoms in women who were fitted successfully with a pessary for pelvic organ prolapse. Am J Obstet Gynecol. 2004;190:1025.
Hagen S, Stark D, Maher C, Adams E. Conservative management of pelvic organ prolapse in women. Cochrane Database Syst Rev. 2, 2004. CD003882
Jelovsek JE, Maher C, Barber MD. Pelvic organ prolapse. Lancet. 2007;369:1027.
Lentz GM. Anatomic defects of the abdominal wall and pelvic wall. In: Katz VL, Lentz GM, Lobo RA, Gershenson DM, editors. Comprehensive Gynecology. 5th ed. Philadelphia: Mosby/Elsevier; 2007:513.
Sulak PJ, Kuehl TJ, Shull BL. Vaginal pessaries and their use in pelvic relaxation. J Reprod Med. 1993;38:919.
Thakar R, Stanton S. Management of genital prolapse. BMJ. 2002;324:1258.
Zeitlin MP, Lebherz TB. Pessaries in the geriatric patient. J Am Geriatr Soc. 1992;40:635.
[/level-membership-for-obstetrics-gynecology-category][not-level-membership-for-obstetrics-gynecology-category]
Chapter 249 Pessary Fitting
